
- Author / Uploaded
- Mury Rabin
Art therapy and eating disorders: the self as significant form
Art Therapy and Eating Disorders Art Therapy and Eating Disorders The Self as Significant Form Mury Rabin Columbia Un
1,988 44 2MB
Pages 248 Page size 335 x 503 pts Year 2011
Recommend Papers









File loading please wait...
Citation preview
Art Therapy and Eating Disorders
Art Therapy and Eating Disorders The Self as Significant Form
Mury Rabin
Columbia University Press
New York
Columbia University Press Publishers Since 1893 New York Chichester, West Sussex
Copyright © 2003 Mury Rabin All rights reserved Library of Congress Cataloging-in-Publication Data Rabin, Mury. Art therapy and eating disorders : the self as significant form / Mury Rabin. p.
cm.
Includes bibliographical references and index. ISBN 0-231-12768-5 (cloth : alk. paper) — ISBN 0-231-12769-3 (pbk. : alk. paper) 1. Art therapy. 2. Eating disorders—Treatment. 3. Body image disturbance— Treatment. 4. Self. I. Title. RC489.A7 R33 2003 616.85′260651—dc21 ∞ Columbia University Press books are printed on permanent and durable acid-free paper. Printed in the United States of America c 10 9 8 7 6 5 4 3 2 1 p 10 9 8 7 6 5 4 3 2 1
2002034833
To the individuals who gave up their identity to become subjects in a courageous journey to find their Self
CONTENTS
Acknowledgments
ix
Introduction
xi
CHAPTER 1
Significance of Appropriate Body Image
1
CHAPTER 2
Body Image and the Self
11
CHAPTER 3
The Therapy of Art Therapy
22
CHAPTER 4
Phenomenal and Nonphenomenal Body Image Tasks in the Treatment of Eating Disorders and Other Addictions (PNBIT): The Method
27
CHAPTER 5
PNBIT Clinical Applications
43
CHAPTER 6
Conclusion
151
Afterwords: Toward an Ethical Society
160
APPENDIXES 1
Extracts of Exit Tape Recordings a. Jessica Mason b. Claudia Bernard c. Heather Allen d. Linda Miller
165 165 168 169 172
2
Self Report Form
179
3
Therapist Report Form
181
4
Sequence and Time Chart
183
5
Outline Drawing: Figure Selection, Male
185
Megan Brown’s recording is included in chapter 5.
—
vii
—
viii
— Contents
6
Outline Drawing: Figure Selection, Female
186
7
Body Dimension Estimate and Measurement: Linear, Male
187
Body Dimension Estimate and Measurement: Circumference, Male
189
Body Dimension Estimate and Measurement: Linear, Female
191
Body Dimension Estimate and Measurement: Circumference, Female
193
11
Sandworlds Grid
195
12
Questionnaires
196
8
9
10
a. Eating Questionnaire b. Body Contour Drawing c1. Self Box Questionnaire c2. Comparison of Self Box 1 and Self Box 2
196 200 201 201
13
Medical Release Form
203
14
Medical Questionnaire
204
15
Abstract from “The Yo-Yo in Art Therapy: The Use of Art Therapy in Eating Disorders”
205
16
Art Therapy Images as an Index to Suicide
207
17
Metropolitan Life Insurance Height and Weight Tables and Frame Size Estimate Chart (1983)
209
Abstract from “Phenomenal and Nonphenomenal Body Image Tasks in the Treatment of Eating Disorders”
211
19
The Scope of Art Therapy
213
20
Relationship of Issues in Eating Disorders
215
21
Figure Selection II
216
22
Color Chart
217
23
Tissue Box Estimate
218
References
219
Index
225
18
ACKNOWLEDGMENTS
Art, whatever form it takes—a painting, a story, a poem, a musical composition, a dance—is always a product of the total being who creates it. It incorporates all of that artist’s inner experiences as well as his multiple environments, including all the people who have been on the landscape of his life: his family and his world. All the good and nurturing things are there and all the negative and challenging experiences as well. They enter the prism of his life force and emerge alchemized in his unique vision. Each expands and humbles at the same time. I want to say an awesome “thank you” to the thousands of individuals I have known and whom I treasure. My father’s creative spirit and my mother’s challenges are surely part of this work. My own family, without exception, has been accepting of my dedication and pursuit of each new idea. My art has been the major force that fueled the academic work. My husband, Gideon, and my two children, Brandon and Staton, all authors in their own right, were empathetic, knowing the delicate balance necessary to continue the long and circuitous route, which at times defied the beaten path, on which I found myself. The generosity of the people who mentored me during my years of learning and working: teachers, academic medical universities, colleagues, friends, and, especially, those in need who came for my help, enriched me far beyond the limits of the roles we had. In this new venture, the journey of manuscript to book, I appreciate the professional qualities demonstrated by those at Columbia University Press. I am grateful to John Michel, executive editor, who made it seem possible. His response to my first phone call was a cordial invitation for me to take the first step into the unknown, and he led me gently through the intricacies of the process. Thank you. The staff, especially Susan Pensak, senior manuscript editor, were diligent, patient, and tolerant of my concept. I thank them all. —
ix
—
INTRODUCTION
Art, accompanying man on his difficult journey to himself, has always been ahead of him at the goal. —Carl Jung
The reader who seeks a succinct definition of art therapy will be disappointed. Art therapy applications vary, as any therapy, according to the individual who presents with a particular problem to a therapist who will direct treatment methods applying to that person at a particular time, in a particular setting. Treatment that is based on the definition of a syndrome documented in the Diagnostic and Statistical Manual of Mental Disorders (DSM), which provides guidelines and a number for each disorder, often limit the critera for diagnosis. In the push for efficiency and economy, hospitals are reimbursed for treatment based on these factors and have adhered to the guidelines in the DSM by limiting the number of in-hospital stays allowed for a particular syndrome. The number of private therapy sessions is also restricted. This approach to treatment does not serve all patients. This book focuses on a method used with obese and anorectic women who were in crisis at the time of entry into the project. The manual (see chapter 4) describes a series of tasks and how to apply them. The case studies (see chapter 5) report on how these tasks served each participant. In traditional treatment programs the addictive problem has been addressed by treating the symptom directly, e.g., for the alcoholic: going off alcohol, for the obese: dieting, for the anorectic: eating more, etc. Where a patient has succumbed to a drug overdose, or for the obese or anorectic in a medical emergency or state of crisis, hospitalization and observation are, of course, necessary. The symptom is not the cause but the result of a missing self-concept. The writer’s experience with each of these populations revealed a common thread—low self-esteem. It was expressed by denial, anger, defiance, perfection. Each of the individuals covered up his identity. The need to identify, recognize, and acknowledge the self-concept comes before self-esteem, positive or negative. The tasks are designed to be a preamble to treatment of the symptoms. Art therapy —
xi
—
xii
— Introduction
includes both verbal and nonverbal work. The two hemispheres of the brain are involved. The tasks require the active participation of the client and include crossing the corpus callosum, from right hemisphere activity to left hemisphere activity for each session. While each of the tasks appears to be different, each is really addressing the same problem at each session. Each task reveals a different aspect of the self. It is the repetition of this goal that reveals the truth. Today’s art therapists have evolved into a complex body of clinicians working in an array of settings. The roots of art therapy began with the introduction of art into the regimen of patients in hospitals, nursing homes, and other institutions that served a wide range of populations. These early programs were activity projects run by volunteers and provided patients with an opportunity for socialization in the facility. They served also for staff to observe the patient’s ability to function physically and mentally. The connection from the art to any value or use other than participation was never explored. The introduction of the use of art as a therapeutic tool was defined in Margaret Naumburg’s Dynamically Oriented Art Therapy: Its Principles and Practice (1987). She writes: The process of dynamically oriented art therapy is based on the recognition that man’s fundamental thoughts and feelings are derived from the unconscious and often reach expression in images rather than in words. By means of pictorial projection, art therapy encourages a method of symbolic communication between patient and therapist. Its images may, as in psychoanalytic procedures, also deal with the data of dreams, phantasies, daydreams, fears, conflicts and childhood memories. The techniques of art therapy are based on the knowledge that every individual, whether trained or untrained in art, has a latent capacity to project his inner conflicts into visual form. As patients picture such inner experiences, they frequently become more verbally articulate. (p. 1)
Naumburg expands on how verbalization may affect the progress of treatment: Art therapy is not opposed to verbalization, which it uses in combination with spontaneous art production, but it has been shown that patients become able to associate freely in words to the spontaneous images they have created, and this leads inevitably to a speeding up of the therapeutic process. (pp. 3–4)
Introduction — xiii
Though many approaches were based on Naumburg’s original work and developed into structured academic programs, others that followed became the product of particular art therapists whose practice was defined by the different populations they served. Like the medical profession, which no longer offers a general internist, once known as the family doctor who made house calls, art therapy is now multidimensional in its scope. It serves a wide variety of individuals including patients who are not hospitalized and who range from very young children to the aged and dying. Art therapists have adapted to situations of crisis, serving as special counselors in emergency situations to individuals and groups. Trained and credentialed, art therapists have not been welcomed by the therapeutic community. Artists are not viewed as disciplined, hardworking, or focused. A reticence by other therapists to accept art therapy as a legitimate discipline may stem from a feeling that art therapy is not traditional enough to trust. It is hoped that this text will dispel that fear and encourage other clinicians to embrace its methods. This book is designed to be used by all professionally trained clinicians. It invites them to open their creative corridors to apply a new approach to treatment of addictive disorders. The work is dedicated to the idea that all therapists are connected to each other. Therapists who use mainly verbal treatment have nonverbal components present in their work. The ambience of their office, their own appearance and manner, the arrangement of time, are all nonverbally present in the session; the verbal therapist is impacted in turn by the appearance, manner, and participation in the session of the patient. All the nonverbal elements factor into a process that is mainly verbal. In much the same manner, the art therapist is impacted verbally in important ways during a session that is mainly focused on the nonverbal, i.e., drawing, clay work, weighing and measuring the body. All these are accompanied by the intervention of important verbal exchanges. The ability of the patient involved in art therapy to express herself in words is vital to her ability to participate in her life. The two parts must be developed together. The reader will see how this is accomplished in the application of the tasks (see chapter 4). Right and left brain hemisphere activity is the key to illumination, healing, and growth.
Art Therapy and Eating Disorders
CHAPTER 1
Significance of Appropriate Body Image
Art Therapy in the Twenty-first Century This book explores the use of phenomenal and nonphenomenal body image tasks as therapeutic treatment in anorexia nervosa and obesity. Treatment measures for these syndromes have been major topics of theory and research in recent years as these and other eating disorders have increased in frequency and even impacted on young children. There has been general failure to find lasting solutions to management of these intractable conditions, which have a high rate of morbidity and mortality (Weiner 1985). The author’s interest in these concepts developed while working with groups of chronic alcoholic and drug-abused patients as well as those with eating disorders. The clinical evidence was compelling in identifying an addictive quality common to these various problems. Hatterer (1980) addresses this idea: I do not believe that any one addictive personality type exists, but that people become addicted because they are vulnerable to the addictive process, which is rampant in our culture. . . . Today we extend the concept of addiction . . . not only to drugs or alcohol, but to food, smoking, gambling, buying, or some form of work, play or sex. I believe that all these addictions have a common denominator, which is a process that depends on constitutional, family, peer, environmental, and sometimes genetic,
—
1 —
2
— Significance of Appropriate Body Image
physiologic, chemical and ethnic factors, and which serve one or several functions in a person’s adaptation to life. (pp. 15–16)
Hatterer’s concept that the abuse of food may be a function of the addictive process is supported by studies by Dole at Rockefeller University. He observed that the tendency of obese patients to relapse after dieting resembled the tendency of cigarette smokers and heroin addicts to relapse even after long periods of abstinence. He concluded that relapses among some obese patients have a metabolic biochemical origin. Hatterer’s and Dole’s view of eating disorders as addictive in quality is borne out by the work of Marrazzi and Luby (1986). They state, “Endogenous opioids may play a homeostatic role in appetite regulation in humans at both ends of the spectrum (pp. 193–194). They conclude: Chronic anorexia seems unresponsive to the spectrum of psychotherapies. Current psychological hypotheses . . . are of limited utility in reversing its course when it has stubbornly persisted for years. . . . An auto-addiction model may not only provide a basis for further biological research but contribute to alternative therapeutic approaches as well. (p. 202)
This work is focused on the method used with individuals who have suffered with eating disorders. Chapter 5 details the case studies of five women, two anorectic and three obese, who completed the protocol described in chapter 4. Chapter 4, “Phenomenal and Nonphenomenal Body Image Tasks in the Treatment of Eating Disorders (PNBIT): The Method,” is presented in the form of a manual for the use of a therapist working with individuals who are affected with these syndromes. The PNBIT can be used by a therapist who works primarily with verbal means. Where the therapy appears to be static, the application of some or all of the tasks can move the patient/client toward self-management, healing, and growth. Following are some definitions of terms used in the text: Body image: The picture of our own body that we form in our minds (Schilder 1953). Bruch (1973) defines it as “a plastic concept which is built from all sensory and psychic experiences and is constantly integrated in the central nervous system. Underlying it is the concept of Gestalt, which sees life and personality as a whole” (p. 87).
Significance of Appropriate Body Image — 3
Combined phenomenal and nonphenomenal task: Body Contour Drawing (BCD). See chapter 4. Nonphenomenal body image: A term used to denote the individual’s unconscious and symbolic expression of the self acquired over time through interpersonal relationships. Nonphenomenal tasks: 1. Chromatic Family Line Drawing (CFLD), 2. House/ Tree/Person/Person/Animal (HTPPA), pencil and chromatic, 3. Mandalas (M), Body Image and Self Image, 4. Sandworlds (SW), 5. Self Box (SB), 6. Kinetic Family Clay Sculpture (KFCS). Normal weight: A term used to denote weight in pounds plus or minus five percent of the normative weight for age and height as designated in current medical weight table. Phenomenal body image: A term used to denote the individual’s direct and conscious awareness of the body as an objective physical entity, based on sensory experiences, involving sight and touch, focusing on weight, form, mass, coloring, and measurements of length and breadth of the body boundaries. Phenomenal tasks: 1. Weighing of individual on scale, 2. self-viewing in full-length mirror, 3. self-analysis through touch and other sensory input, 4. Body Dimension Estimates and Measurements (BDEM). PNBIT: Phenomenal and nonphenomenal body image tasks, i.e., the group of eleven items administered to the individuals in chapter 5. (For a complete description of tasks see chapter 4.) Self: “The psychophysical total of the person at any given moment, including both conscious and unconscious attributes” (Hinsie and Campbell 1970). Self-concept: The whole range of complicated attitudes and fantasies an individual has about her identity, her life role, and her appearance. This is in contradistinction to attitudes an individual expresses about herself verbally. It is assumed some of the most important of the individual’s selfconcepts are either so unpleasant to face or are acquired at such an early preverbal period as to be unavailable for conscious reporting (Fisher and Cleveland 1968). Self-esteem: The appraisal or value the individual sets on the self. TSCS: Tennessee (Department of Mental Health) Self Concept Scale, a pencil and paper verbal measure of self-concept. The scale consists of one hundred self-descriptive statements the subject uses to produce a verbal picture of herself.
4
— Significance of Appropriate Body Image
Yo-yo syndrome: Chronic condition affecting an individual which manifests itself in episodes of alternative bingeing and dieting as a means of gaining and losing weight.
There is no way to understand how art therapy works without connecting it to the making of art. The search for meaningful form is one of the primary goals in psychotherapy. Persons in analysis . . . are struggling with their world—to make sense out of nonsense, meaning out of chaos, coherence out of conflict. They are doing it by imagination, by constructing new forms and relationships in their world, and by achieving through proportion and perspective a world in which they can survive and live with some meaning. (May 1975:125)
If a nonhealth or pathological state is defined as having the quality of disturbance or disorder in one’s life, then a state of health may be defined as that which moves toward ordered form. Rogers said, “Man’s behavior is exquisitely rational, moving with subtle and ordered complexity toward the goals his organism is endeavoring to achieve” (1961:194–195). This idea is emphasized by May (1975): Our passion for form expresses our yearning to make the world adequate to our needs and desires, and, more important, to experience ourselves as having significance. . . . Insights emerge not chiefly because they are “intellectually true” or even because they are helpful, but because they have a certain form, the form that is beautiful because it completes what is incomplete in us. . . . This new form that suddenly presents itself, comes in order to complete a hitherto incomplete Gestalt with which we are struggling in conscious awareness. (p. 132)
Such a process involves organismically selected direction that allows psychological freedom within prescribed limits set by the inner and outer environments of each individual. One may see a parallel here from psychological form to art form. Writing in 1913, Bell (1958), the English critical theoretician of art, revolutionized the study of all the arts by his concept of form: For either all works of visual art have some common quality, or when we speak of “works of art” we gibber. . . . What is this quality? . . . Only one answer seems possible—significant form. In each, lines and colours
Significance of Appropriate Body Image — 5
combined in a particular way, certain forms and relations of forms, stir our aesthetic emotions. (p. 17)
He continues, “These relations and combinations of lines and colours, these aesthetically moving forms, I call ‘significant form’ and Significant Form is the one quality common to all works of art” (p. 18). Langer (1957) reevaluated and expanded on Bell’s original concept: Artistic form is congruent with the dynamic forms of our direct sensuous, mental, and emotional life; works of art are projections of “felt life,” as Henry James called it. . . . A work of art expresses a conception of life, emotion, inward reality. . . . It is a developed metaphor, a nondiscursive symbol that articulates what is verbally ineffable—the logic of consciousness itself. (pp. 25–26)
She continues: A work of art is an expressive form created for our perception through sense or imagination, and what it expresses is human feeling. . . . One quality shared by all good works of art is “significant form” . . . structure, articulation, a whole resulting from the relation of mutually dependent factors or more precisely, the way that the whole is put together. (pp. 14–16)
And Langer concludes: The more you study artistic composition, the more lucidly you see its likeness to the composition of life itself, from the elementary biological patterns to the great structures of human feeling and personality that are the import of our crowning works of art; and it is by virtue of this likeness that a picture, a song, a poem, is more than a thing—that it seems to be a living form, created, not mechanically contrived, for the expression of a meaning that seems inherent in the work itself: our own sentient being, Reality. (p. 58)
Analysis of the art productions of the individuals who participated in the case studies detailed in chapter 5 reveals that when the art approached the significant form of aesthetic art, it was also an index to the state of the psychological health of the person at the time it was made. A comparison of the quality of a task done at the outset of treatment and repeated later demonstrates the individual’s ability to improve her aesthetic art expression.
6
— Significance of Appropriate Body Image
Improvement in the state of the individual’s ability to function, to self-manage, was achieved over time. But illumination and truth were revealed along the way, by their courage in facing their truth and being willing to give up denial. One woman was asked what art therapy did for her. She said, “I learned that my words didn’t match my pictures.” Perhaps this is as good an explanation of the dynamics of art therapy as any other. In a person’s search for the Self, he is seeking congruence between what he is as a physical entity and what he is as a psychological entity. Repeated episodes of gaining or losing weight may be an effort to find the right dimension for the Self through the measure of the physical body and its relationship with the rest of the world. The universal genetic template of the human form may act internally as the constant against which the everchanging concept of body image of each individual refers. The obese and anorectic may suffer disorder when this archetypal form is violated. The person is pulled or pushed (gaining or losing weight), irresistably drawn toward stabilizing the body boundaries, as they are both personally and collectively defined in human terms, in an effort to reestablish its gestalt. This book offers a manual defining a system of prescribed tasks. The tasks invite the active participation from the client. She creates a visible, tangible, permanent record of her response to each task. Its permanency in its original form is its unique quality. This allows both the client and therapist the opportunity to reflect and review the work at a distance in time from its making. It also provides a way of comparing the state of the client from the first rendering of a task to the same task done at a later time. Art therapy taps into the unconscious, no matter how attentive and focused the client was when working on the task. Art therapy productions, like dreams, contain manifest as well as latent material. I call these solar dreams. The subject drawn is the manifest material, but everything else, i.e., color, placement on the page, emphasis, omission, title, signature, etc., represents the latent or unconscious content.
American Body Image: Fat and Thin More than twenty years ago the body of the ideal woman in the United States was supposed to resemble the then current British young
Significance of Appropriate Body Image — 7
fashion model named Twiggy. Her figure appeared to be that of a prepubescent girl whose body had not yet developed breasts or other features associated with the normal growth of a young woman. Thin, and thinner, was in and became the national standard for beauty of women’s bodies. Styles of clothing reflected the trend of the slim childlike figure: short straight skirts and shirts designed to deemphasize the more abundant form. Department stores limited their inventory of apparel for large women. What little was available was usually confined to a small area, often situated in the basement near the ladies lounge. For some the focus on measures to reshape the normal female body dimension was sought through diet and exercise. The goal was to achieve the appearance of extreme thinness that was being promoted in the media. Celebrities were seen to be replicas of each other—and this fueled public adoration of the image. The public was shocked to learn that it was also life threatening. The practice of extreme measures to limit food intake was identified as anorexia. Karen Carpenter, the popular young singer, died of the addictive abuse of these practices. The 1980 Diagnostic and Statistical Manual of Mental Disorders (DSM-III) listed Anorexia Nervosa as a subclass of Infancy, Childhood, or Adolescent Disorders, number 307.10, giving it legitimacy in the lexicon of psychiatric diagnoses. Anorexia was defined as follows: A. Intense fear of becoming obese, which does not diminish as weight loss progresses. B. Disturbance of body image, e.g., claiming to “feel fat” even when emaciated. C. Weight loss of at least 25% of original body weight or, if under 18 years of age, weight loss from original body weight plus projected weight gain expected from growth charts may be combined to make the 25%. D. Refusal to maintain body weight over a minimal normal weight for age and height. E. No known physical illness that would account for the weight loss. (p. 69)
While some thought that anorexia was a new syndrome, the medical community was aware that only the publicity about it was new. In his book Holy Anorexia Bell (1986) documents the existence of anorexia as early as the fourteenth century. It was a known practice of nuns. The Italian
8
— Significance of Appropriate Body Image
medieval saint, Catherine de Siena, died from recurring anorectic episodes that had begun at an early age. Information about the rituals of fasting, limited intake of food, use of laxatives, enemas, and self-purging became widespread. First-year college coeds (especially in women’s colleges) were inducted into these practices by older students, like entering into a secret sorority. Anorexia became rampant on campuses. Only when the residence halls’ plumbing became clogged from overload of vomiting purges did the administration grow aware and alarmed. Yet little was done to inform parents or provide programs to assist the affected students. Some hospitals created in-hospital units for patients with chronic anorexia. Treatment in these special units involved monitoring of patients to assure they ingested an appropriate amount of prescribed balanced diet at mealtimes. Therapy was focused on the symptom, i.e., eating. The goal: to have the patient gain enough weight to reestablish normal body functions. While all this emphasis on slender bodies had been in the news, an old problem—obesity—had become a national emergency, its incidence having escalated in the United States. More adults than ever were at risk of succumbing to the serious physical dangers already known. Health alerts warning of the risks of obesity had been shared by doctors with their patients for many years. Heart attacks, diabetes, and stroke are only some of the many serious problems attributed in part or whole to the dangers of overweight as well as obesity. Now a new and alarming statistic was added, i.e., children had become obese at a younger age than had been previously identified. Dr. Richard Satcher, the U.S. surgeon general, declared obesity to be “epidemic in our country.” Programs abound that address the obvious symptom of obesity, i.e., weighing too much by standards set for height, weight, age, sex, and body type. Diets designed to guide the individual toward achieving a recommended weight have been advocated by every possible means. Exercise programs at home and in the gyms, in groups or alone with a private trainer, are available in every community. Overeaters Anonymous (patterned after the well-known Alcoholics Anonymous), Optifast, Nutrisystem, Jennie Craig, and Weight Watchers have become familiar through advertising and with promotion by well-known public figures. A recent
Significance of Appropriate Body Image — 9
addition, Zone, will deliver balanced diet meals to your door, including snacks. This is reminiscent of the program for incapacitated housebound seniors called Meals on Wheels. Herbs, meditation, hypnosis, and aromatherapy are some of the other weight control measures available. Once rare, and considered risky by some, the popularity of bariatric surgery increased, with numbers of individuals opting for this process. While recent reports have come out as more critically favorable for this and other surgical procedures, difficulties in aftercare as well as death have also been reported. On the surface anorexia and obesity seem to be antithetical. Yet when viewed on a continuum the two disorders touch, as the eating cycles of each mimic each other in the classic yo-yo syndrome. The anorectic has periods of starving and bingeing as the obese has periods of gorging and dieting. Such manipulation of body dimension through inappropriate ingestion patterns places inordinate stress on the metabolic and hormonal systems. Followed through, for the obese, diets work. It’s simple: eat less, the body metabolizes slower, and one loses weight. Knittle (1972), one of the primary medical researchers in the field, reflects on the futility of such an approach to treatment of obesity. “The simplest and yet the most complex of all disorders: simple in that, in the adult, all that is required is caloric restriction, and complex in that cellular, metabolic, socioeconomic, cultural, and psychological factors all militate against the maintenance of the reduced state” (p. 1055). For the anorectic, too, it would seem that the solution should be simple. Eat more, the body will resume better metabolic function, and one gains weight. Bruch (1973) notes, “Anorectic patients may gain weight for many reasons, or they may seem to make progress in psychotherapy. Without a corrective change in their body concept, improvement is apt to be only temporary” (p. 252). Bruch emphasizes this idea: “A realistic bodyimage concept is a precondition for recovery in anorexia nervosa” (p. 90; my emphasis). Bruch extends her analysis of distortion in body image to the obese as well, noting that weight loss alone will not solve their problem. She states, “Little therapeutic progress can be made unless the abnormal appearance is perceived and acknowledged” (p. 91).
10
— Significance of Appropriate Body Image
It has been estimated that 95–97 percent of obese who go on diets and lose weight regain the weight, and more. Released from observation, the anorectic becomes more resourceful in concealing her problem from family and friends. She will dress in large-size clothing and devise eating patterns that hide the fact that she is emaciated, not eating, and continuing to lose weight. There is a dilemma in our culture. We are overwhelmed with articles and ads that promote maintenance of the tenets of healthy living. At the same time, the pursuit of thinness is underscored by Hollywood celebrities, video and music personalities who display the latest fashions on sylphlike bodies. It is of course both legally and politically correct to accept obese people in the mainstream. Now obese feel they have the right to be fat. Organizations that advocate fat in the workplace and in social settings have made an impact. Clothing stores have transferred their large-sized women’s apparel to the main floor and renamed the whole size category to include large, larger, and “plus” sizes. The conflict continues. Recognition of the advent of the larger woman is acknowledged by signature designers. A formerly super-thin model can now walk on a fashion runway as a fleshy model for large women. Nevertheless, the viewer is challenged to appreciate the impact. Why this conflict continues, when all the evidence suggests that either road is an avenue to debilitating mental and physical health, will be explored in the following chapters. My clinical experience working with individuals who suffer from eating disorders and other addictions has informed me of some of the critical omissions in treatment. Through these experiences I have assembled a series of tasks that help the victim to identify the problem, i.e., a missing link—self-concept—as the preamble to successful self-management.
CHAPTER 2
Body Image and the Self
Seeking the Self From the day of birth, when a baby cries and is picked up and fed, she experiences this as both satisfying and pleasurable. She makes the connection between the physiological and psychological elements related to feeding, which becomes a lifetime scenario for nurturing. In the normal course of development the child ultimately learns to feed herself. The obese and anorectic have not developed, or may have lost, the ability to self-nurture; they eat but do not feed themselves. Never satiated, both become people who eat and continue to cry. The bodily response to caloric restriction is the same whether it is initiated by the anorectic who is starving herself or by the obese who is dieting. These events result in lowered metabolic rate, a conservation of energy. When the anorectic succumbs to a binge, or the obese regains the weight, the body may become less efficient in its response. The constant yo-yoing between eating and not eating, gorging and purging, creates havoc within. Through this polarity people who suffer from eating disorders may cross over from one syndrome to another and become chronically addicted to the process. This creates feelings of failure and lowered self-esteem. Efforts to increase the long-term success of the myriad programs available have been disappointing. Little has been focused on the underlying —
11
—
12
— Body Image and the Self
problem that manifests itself in the physical symptom. None of the various programs has found the formula for authentic management of these insidious problems. While treatment that addresses the symptom may appear to be successful, inevitably, either the syndrome will reappear or transfer from one addiction to another. A common example is the complaint of individuals who give up smoking only to gain weight. As Hatterer (1980) and others have observed, addiction of one kind is part of a process that includes many different versions, licit and illicit. Until the person becomes an active participant in his treatment team, he will not be able to assume responsibility for self-management of his problem. The term self-management is the key. Unlike programs that declare the person to be helpless and in the grip of the addiction, he must be given the tools to care for himself. The symptom will not be managed until the person is able to identify himself. Self-esteem, positive or negative, cannot be assessed until the person’s self-concept is known to himself. This is a preamble to treatment of the symptom. Self-help groups that support the person who is having the problem often result in sustaining the problem.
Body Image Distortion Both anorectic and obese people demonstrate body image distortion. Each may never have developed the sense of the Self or may have lost the ability to know his self-concept. Rose (1981) quotes Kubie (1953) on the developing child’s first awareness of the Self as an enduring frame of reference. The body is the model according to which we construct the world as a whole. It provides the original set of coordinates to which we continually return and refer during the course of development. . . . The first learning concerns itself with bodily things. . . . We establish lifelong symbolic connections between our own body and the outside world. (p. 98)
It is an astonishing experience to be in the presence of an anorectic, 5-feet-8-inches tall and weighing 103 pounds, who looks at herself in a fulllength mirror and sees herself as fat. Some anorectics will identify particular parts of their bodies as having “lumps of fat.” Obese individuals also demonstrate their inability to identify their own body while viewing them-
Body Image and the Self —
13
selves in the mirror. Some may see a thinner person and some imagine the body to be much larger than it actually is. Of course, the mirror reverses the image and also reduces the image to one-half the actual size, no matter how large the mirror. This often comes as a surprise to the average person. We never think that we are not our normal size when reproduced in a mirror. Gombrich (1960) urges the reader to make the following experiment in a steam-clouded bathroom mirror: It is a fascinating exercise in illusionist representation to trace one’s own head on the surface of the mirror and to clear the area enclosed by the outline. For only when we have done this do we realize how small the image is which gives us the illusion of seeing ourselves “face to face.”
He continues: “To be exact it must be precisely half the size of our head . . . since the mirror will always appear to be halfway between me and my reflection, the size on the surface will be one-half of the apparent size.” He concludes: “But however cogently this fact can be demonstrated with the help of similar triangles, the assertion is met with frank incredulity.” Accurate body image is necessary for the total and independent functioning of the individual. It is important in relation to everyday tasks but also in the maintenance of a stabilized body dimension. Here it is critical. The body image or the body identity is the conceptualization of the body’s structure and functions that grow out of the awareness of the Self and one’s body in action. Schizophrenic children are often deficient in the ability to localize, discriminate, or give pattern and meaning to body perceptions. “Thus they lack body images that are integrated, stable in time, and clear in form. One child walked about all day feeling her body. . . . An alcoholic crouched in a fetal position may need to get in touch with his body” (Goldfarb 1964). Where methods of treatment for the symptoms of eating disorders are focused on correcting the symptom, success for long-term maintenance of the corrected state, has been abundantly disappointing. Where body image connection is impaired or distorted it is necessary to restore and repair body dimension concept as a prerequisite to treatment of the symptom. Following this process, the individual becomes an active member of his treatment team. The body image cannot be assessed until the
14
— Body Image and the Self
self-concept is given stable life. Where the self-concept is unavailable the individual is confused about her body image. Body image is organized over the years, primarily on the basis of incoming kinesthetic and tactile perceptions. Self-concept includes perceptions, thoughts, and feelings experienced by the ego in reference to viewing its own body. Both these functions contribute to accurate visualization of the physical self. For mature thinking, virtual image in the mirror needs to be translated into a proper symbolization of the bodily self (see the section in chapter 6, “From Sign to Symbol”).
Eating Disorders: Not Just a Woman’s Problem Although the subject of eating disorders has been given attention in the media as well as in the research laboratories, very little documentation of the incidence in males has been assembled. Part of the reason for the limited material is undoubtedly due to the fact that eating disorders have always been described as a “woman’s problem.” In my experience working with drug and alcohol addicted males, eating disorders emerged without official labeling of the syndrome. Men did not want to be identified with a woman’s disorder. Close examination of the histories of these individuals revealed that the etiology was not the same, but the assault on the body justified identifying it as an eating disorder. Recent studies based on research with male college students concluded that the men, as the women, had a body image distortion, emerging from a variety of pressures (Anderson 1990). A more recent exploration of body image distortion in males is developed in The Adonis Complex (Pope, Phillips, and Olivardia 2000). The authors identify four areas they call hidden signs and symptoms of the Adonis complex: weightlifting and exercise compulsions, body dysmorphic disorder, eating disorders, and steroid abuse.
September 11, 2001 A dramatic and recent event dating from the World Trade Center disaster in New York City on September 11, 2001, has resulted in a
Body Image and the Self —
15
switch described in the following report of July 3, 2001, in the New York Times that covered the Spring 2002 men’s fashion shows. A drastic change was seen on the runways: “Suits created from damask made the (male) models look like ambulating napkins.” Ginia Bellafonte developed her review of the fashion scene: Designers seemed content to ignore the idea that men might ever want to present themselves as virile, purposeful and grownup. For years men’s shows have celebrated cartoonish archetypes of masculinity as rendered in pornography, gay and straight. . . . This season, however sexuality of any sort was scarcely in evidence, and swimwear barely turned up. . . . Swim trunks were shown on a reed-thin model and paired with a sweater. . . . Trunks appeared with a robe on the skinniest model in the show.
Bellafonte continued: The male form idealized by fashion right now is one in which limbs are needlelike—body-fat ratios rest at approximately 4 percent. . . . Suits revealed chests as concave as saucers. . . . The attentuated male body has long been championed at Prada. . . . Models, as always, were boys, the vacant-eyed kind who look as if they do nothing more than bring their mothers the morning newspaper. . . . This time, though, the models were not even dressed to resemble pretend adults. ... A trend at other runways gave a feminizing impression. . . . The look also tended toward a kind of sexlessness.
The article noted a remark by a twenty-four-year-old model that he was getting far less work this season than last and had been told that he was “too big.” The tragedy at the World Trade Center focused on the heroic efforts and ultimate loss of life on the part of the New York City fire and police departments. The TV coverage of the work at Ground Zero showed many portraits of these legitimate heroes. Their pictures appeared in major magazines and on the front pages of newspapers around the country. Now the American male body image of a “manly man,” vigorous and robust, was the preferred form. Once again the male body image is reversed. Betty Friedan’s groundbreaking book The Feminine Mystique (1963) opened a new era of defining women’s legal and social inequalities in the United States. Friedan’s work spawned a large following of writers and
16
— Body Image and the Self
activists who added their voices to what was called the women’s movement. It began a struggle to enunciate and resolve the many differences in mores of marriage, business, and social relationships between women and men that continues to the present. The feminist movement became a force that touched the very essence of women and men, stirring male and female qualities within each individual. The movement precipitated a battle that developed into a gender hodgepodge: women against men, men against women, and women against women. Ultimately, the struggles of men against men, in public wars in the past, involving power, now became more personal. What is being played out is the old anima/animus within. The conflicts of each person in a search to find him or herself, indeed, the Self, is at the heart of the matter of feminism: women finding their balance using the movement as a vehicle for action. This involved both sexes and their relationship one to the other. More important to resolve is the potent reaction to the same sex, as it is the embodiment of the Self. Throughout the sixties, and beyond, it became politically correct to support Friedan’s revolutionary ideas. Writers contributed by exploring many facets of the problem. Gloria Steinem (1995) notably added her innovative voice. She related her adventure in undercover reporting. Using a false identity, Steinem applied for and was hired to be a Playboy bunny in Hugh Hefner’s Playboy Club in New York. She kept a diary and published a report of her experiences in the club, documenting the indignities endured in one month (January 24, 1963–February 27, 1963) of life as a Playboy bunny. Though her article received positive responses, it was also followed by death threats and lawsuits (p. 75). The old boundaries of gender stereotypes were altered; a new feminism emerged. It became a case-by-case process: each woman defining issues in personal terms as well as in a national idiom. Steinem wrote, “Finding language that will allow people to act together, while cherishing each other’s individuality, is probably the most feminist and truly revolutionary function of writers” (1995:4), and observed, “Better to be one’s whole self than be immortal” (p. xxi). Today there remains a backlash against equality and valid change for men and women. One of the many issues addressed is the conflict between anti-abortion and pro-choice groups. Violence that resulted in murder and
Body Image and the Self —
17
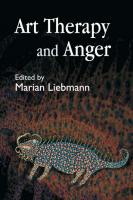
attempted murder did not quell those in opposition to the feminist movement. Asked to define it in 1992, an ultra-right-wing talk show host compressed feminists with Nazis in a single word: feminazi (see Steinem 1995). There have also been critics, including Hoff Somers (1995), Chesler (2001), and Estrich (2001), among others. Reflecting on her experience in 1963 as a Playboy bunny, Steinem has remarked that she realizes “all women are Bunnies” (1995). Throughout history there have been political, social, and cultural issues that have focused on women. Women’s voting rights, achieved in 1920, followed by the so-called flapper era, which centered on dress and social behavior, were moves to break away from old stereotypes in relationships between women and men. None, however, had the long-lasting and wide-ranging impact of what began in the sixties with the publication of Friedan’s Feminine Mystique. Though the feminist movement raised the consciousness of the country about women’s roles in the political and cultural life of the United States, it did not resolve the inner conflicts that were aroused in both sexes. Unless there is inner reconciliation to balance all the factors in one’s life, male or female, the individual will continue to struggle. The search for the Self requires the opposing psychological forces within to establish a balance between the push and pull of the anima and animus. The yo-yo syndrome is often used to describe the ebb and flow of gaining and losing weight in an individual affected with an eating disorder, anorexia or obesity. When a female anorectic has lost a significant amount of weight, her body becomes more lean. Her body appears to have a more masculine aspect. In males, as they gain weight and become obese, fat deposits are evident in the hips and breasts, giving them a more feminine aspect (see figures 2.1 and 2.2). Exaggeration of the natural appearance of the gendered form destabilizes the boundaries of the body dimension and results in an amorphic body image. Manipulation of the physical body boundaries challenges the genetic template of the human form, creating a struggle to reestablish its gestalt. Continued yo-yo cycling can result in a permanent body image distortion and an increase in the obsessive addiction to the process. In her introduction to a recent edition of The Feminine Mystique (2001), Anna Quindlen acknowledged Friedan’s powerful impact on the social,
18
— Body Image and the Self
Bulimia
Anorexia
Obesity
NORMAL WEIGHT Figure 2.1
—
Female Figure: Range of Weight Levels
cultural, and political institutions of the nation. She noted “a certain feeling among smug overachievers of the post-mystique generation that time had passed the book by, that we had moved away from the primer into the advanced course in seizing control of our own lives” (p. xxi). She affirmed its current relevance: “It was prescient, and it continues to be so” (p. xii). In this same edition, Friedan added an epilogue: The more I’ve become myself—and the more strength, support, and love I’ve somehow managed to take from, and give to, other women in the movement—the more joyous and real I feel loving a man. I’ve seen great relief in women this year as I’ve spelled out my personal truth: that the assumption of your own identity, equality, and even political power does not mean you stop needing to love, and to be loved by, a man, or that you stop caring for your kids. I would have lost my own feeling for the women’s movement if I had not been able, finally, to admit tenderness. . . . I think the energy locked up in those obsolete masculine and feminine roles is the social equivalent of the physical energy locked up in the realm of E = MC2—the force that unleashed the holocaust of Hiroshima. I believe the locked up sexual energies have helped to fuel, more than anyone realizes, the terrible violence erupting in the nation and the world during these past ten years. . . . The sex-role revolution will liberate these ener-
Body Image and the Self —
19
Bulimia
Anorexia
Obesity
NORMAL WEIGHT Figure 2.2
—
Male Figure: Range of Weight Levels
gies from the service of death and will make it really possible for men and women to “make love not war” (Friedan 2001:394–395).
It is interesting to note that Freud and Jung were colleagues and close friends for a period of six years, working together, developing their analytical concepts and advancing their individual theories. The relationship ended because they could not reconcile their differences, especially in regard to the interpretation of sexuality. Nevertheless, each agreed on the importance the role of sexual development plays in the life of both sexes and its significance for the psychic health of the mature individual (Storr 1989). Stevens described Jung’s view: Just as gender is experienced as the archetypal principle appropriate to one’s sex, so relations with the other sex rest on an archetypal foundation. Of all the archetypal systems enabling us to adapt to the typical circumstances of human life, that involved in relating to the opposite sex is the most crucial. Jung called this contrasexual archetype the animus in women and the anima in men. As the feminine aspect of man and the masculine aspect of women, they function as a pair of opposites (the syzygy) in the unconscious of both, profoundly influencing the relations
20
— Body Image and the Self
of all men and women with each other. The anima and the animus act as mediators of the unconscious to the ego, so providing a means for inner as well as outer adaptation. Jung borrowed from biology and applied it to human psychology: The psyche is a self-regulatory system which strives perpetually to maintain a balance between opposing propensities, while at the same time seeking its own growth and development. (1998:53)
Undoubtedly influenced by feminism’s impact on the culture and the changing roles of women, men found themselves displaced from their usual hierarchical position in the family as well as socially and politically. Friedan wrote, “What had to be changed was the obsolete feminine and masculine roles that dehumanized sex.” She added, “Men weren’t really the enemy—they were fellow victims, suffering from an outmoded masculine mystique that made them feel unnecessarily inadequate when there were no bears to kill” (2001:386). Friedan’s noble goal was not realized during the height of the movement. More recently articles and books have appeared that uncover secrets that men have kept from public scrutiny, that is, body image addiction and medical problems related to eating disorders. Usually associated with women, little attention has been given to diagnosis and treatment of these addictive syndromes in males. Men have remained in the gyms, reluctant to come forward to be helped. A new focus on the serious consequences of these insidious problems has finally alerted the medical and clinical communities to acknowledge the life risks at stake. Though books have been written on men with distorted and obsessive body image, including steroid use (Males with Eating Disorders [1990], The Adonix Complex: The Secret Crisis of Male Body Obsession [2000]), there remains resistance to open discussion, treatment, and research of these syndromes for men and boys. The influence of the feminist movement has permanently altered our vision. The “masculine mystique” is on the horizon. The political ethics of a culture are expressed in society by the ebb and flow of visible design in architecture, dress, and city planning. Like art, which is a synthesis of all of the components in a culture, the impact of the political and social state of a community is expressed by the physical surroundings and contemporary appearance of the inhabitants of the culture.
Body Image and the Self —
21
Both men and women are confused about the messages received from a culture that is in transition from one era to another. This confusion is compounded by the impact of family and early educational experiences on the self-concept of the individual. It is likely that this state of the culture has influenced the trend to homogenize men and women. The movie musical, My Fair Lady, based on George Bernard Shaw’s Pygmalion, has Professor Higgins singing, “Why can’t a woman be more like a man?” only to end his refrain: “Like me!” The conflicts between men and women pushing and pulling will not finally, like milk, become homogenized so that the cream will not separate. Men and women can live in harmony, but not to become one another, so that the individual creative forces remain. The plight of men who suffer from a body image distortion has not yet been addressed. Though some have emerged from the gyms and are seeking help, the extent of the problem is still a secret. It is hoped that application of the material in this text will provide relief. The listing of symptoms for a particular diagnosis creates a framework to help the clinician organize treatment and provides a legal means to compensate the parties. It should not be used as a rigid rule to assess the problem of an individual. Addiction is complex and requires a multidimensional approach to treatment. The transfer of addictive syndromes from one to another in both men and women is common—at times so fluid it is hard even for the skilled clinician to identify their boundaries. Treatment, whatever form it takes, must be ongoing and creatively applied. The method of care must engage the patient, who has to establish trust in the therapist so that self-discovery and illumination can be authentically achieved.
CHAPTER 3
The Therapy of Art Therapy
Crossing the Corpus Callosum For a long time researchers believed that the two halves of the brain worked independently of each other. The left hemisphere, considered the more important half, specialized in the activities concerned with verbal and analytical tasks, i.e., speech, writing, and mathematics. The right side housed the emotional and visual attributes, considered a lesser function. Studies in creativity, art, and music have since revealed their contribution to the development of the intellectual function. Thus it is more likely that the two parts work together. Human activity begins a flow across the corpus callosum, the band of fibers that connect the two halves of the brain. This process educates our emotional, artistic side and promotes creative activity in our verbal and analytical side. The verbal and visual become partners, each strengthening the other, interchanging modes with each other, enhancing our total self. Recent radical surgical procedures that involved removal of the left hemisphere of the brain, either the result of accident or recurring epileptic seizure, report that patients transferred activities normally residing in the left side (now removed) to the remaining right side—the right half assuming the role of the left! Techniques of art therapy are based on the knowledge that every individual, whether trained or untrained in art, has a latent capacity to —
22
—
The Therapy of Art Therapy — 23
project his inner conflicts into visual form (Naumburg, cited in Hammer 1958). Its images may, as in psychoanalytic procedures, also deal with the data of dreams, fantasies, daydreams, fears, conflicts, and childhood memories. In spite of the expansion of academic credentialing for programs in art therapy throughout the country, the field has not yet taken its place among established therapies that rely mostly on verbal exchange. This has much to do with each professional being unwilling to incorporate both verbal and nonverbal measures in their protocol of treatment. In the same way that brain research has revealed the connection between both parts of the brain, each therapist must now use a multidisciplinary approach to treatment. Creative avenues must be developed that cross over the corpus callosum, like a bridge to a new landscape. A fresh approach provides a new view to an old problem, encouraging insight and illumination. Close examination of verbal treatment reveals that many of the ways in which art therapy uses a session are already part of the process in more traditional settings. Certainly the patient’s dress, demeanor, and body language are evaluated nonverbally in a verbal session. In an art therapy session words must ultimately become part of the work. In my work I silently observe what the client is doing in the art therapy task. I note many nonverbal aspects, such as the ability to focus, what is done with the presented equipment, i.e., colors, paper, etc. I note in writing the order in which each color is used, changed, omitted, etc. Equally important is the verbal expression used by the client during the process. Upon completion of the art task, each person is asked to sign his name on the production, date it, as well as give it a title and record it in writing on the art. This makes an immediate connection between right and left hemispheres of the brain.
Pictures and Words In working with patients who suffer from eating disorders and other addictive problems, it has been my experience that verbalization is used to cover up denial and is not authentic communication. After completion of the art work I ask the client to describe in words what is in the picture or sculpture. I record exactly what is said, word for word. I
24
— The Therapy of Art Therapy
make no comment or analysis but give the client an opportunity to do this for herself. At times the picture is so provocative that it is better to postpone any further work until a later time. Because art is permanent, it remains in its original state. Having signed, dated, and titled it gives the client an opportunity to view it at a distance in time from its making and to come to it as an objective observer of its meaning. At times, simply looking at the work allows the client to achieve perspective on her own. The most striking effect occurs when the client describes the picture (the manifest dreamlike material) and hears me read back what he said about the picture at the time he produced it, and have him understand that “his words didn’t match his picture.” Over and over in treatment, the client comes to see himself as the “I” he really is deep down. He learns that, at times, the “I” is better than he thought and not necessarily a negative discovery.
Art Therapy and the Unconscious: Solar Dreams Art therapy is truthful; it always communicates. I call it solar dreams. Like dreams, no matter the task, art therapy provides dreamlike material. Dreams are defined as having three parts: the latent dream content evolves from unconscious thoughts and wishes that threaten to waken the sleeper, the unconscious mental operations by which the latent dream content is transformed into the manifest dream is called the dream work, and the third part, the manifest dream, is the conscious experience during sleep, which the sleeper may or may not recall after waking. When we use the term dream we usually refer to the manifest dream. When we speak of the meaning of the dream, it can only signify the latent dream content, i.e., the unconscious content. Dreams come predominantly in visual images. A part of the difficulty of dream telling comes from the fact that the patient has to transpose the picture of the dream into words. In addition, dreams also involve the other senses as well, but they are remembered in pictures. Though Freud made the modern world aware that the unconscious speaks in images, he did not permit his patients to draw their dreams. Yet the dreamer says, “I could draw it, but I don’t know how to say
The Therapy of Art Therapy — 25
it.” Margaret Naumburg notes, “Analysts, psychiatrists, and psychologists have become increasingly aware of the way in which art therapy tends to release deep unconscious material more quickly and, in consequence, helps to speed up the therapeutic process” (p. 513). This is attributed to the immediate translation of inner experiences into pictures rather than words. Art therapy productions contain the manifest material and the latent material all at once. The “dream work” remains permanently available in its original form within the art work. The visual content is the individual’s rendition of the manifest dream, i.e., the picture, she has of the event or the experience she wishes to portray. This is the conscious content. The unconscious or latent meaning is within the picture as well. It is in the use of the page or area enclosed, it is in the colors used, the vigor of application, size, and location of the items in the work. It not only resides in the description of what the picture portrays but in the meaning of the whole production. Psycholanalytic theory is concerned with the normal as well as the pathological. This is also true of art therapy. Unconscious mental processes are of great frequency and significance in normal as well as abnormal functioning. Each psychic event is determined by the ones that preceded it. Nothing happens by chance or in a random way. This is true in drawing. If the drawing comes from the hand connected to the arm, nerves, brain, eyes, it is caused by the person’s totality. In dream studies dreams are often given specific interpretations. In art therapy I have found it to be useful to allow the picture itself, as well as the verbal description of what it is about by the individual, to help both the therapist and the patient to find the ultimate meaning. At times the picture is not only portraying an event or situation from the past but is actually predictive of future events, perhaps lying close to consciousness, ready to emerge. Such pictures have been noted by this therapist and were useful in preventing violent acts to self and/or others. Intervention promptly applied, served the patient by informing and illuminating him to his unspoken—at times, unspeakable—conflicts. Consultation with other members of the treating team provided necessary measures to prevent any harmful actions.
26
— The Therapy of Art Therapy
Art work also is predictive of progress in treatment, which may not be evident in the individuals’ behavior or conscious awareness. This can be a valuable aid in helping the individual to move toward self management. Art therapy is always truthful. It is a potent process. The methods employed can seem very facile; they are often very easy to apply; little equipment is needed to implement a program. It should not be frivolously used with individuals who are not in ongoing treatment with a professionally trained therapist. In her article “The Other Side of Art Therapy” (1979) Gantt emphasizes art therapy’s ability to “tap primary process thinking, bringing into consciousness material that had been unconscious or preconscious (p. 11). In concluding, she warned: It must be cautioned that the use of art and art therapy in an indiscriminate fashion is to be discouraged. To have the art therapy materials simply available or to have them used by a staff member with little or no training in the principles of their therapeutic use is, at the least, to spin one’s wheels or, at the worst, to court disaster. (pp. 17–18)
Where a person has been engaged over time in verbal therapy, perhaps where she has become blocked and unable to progress in treatment, the use of art therapy by the treating therapist can promote a new atmosphere that invigorates treatment. “As patients picture their inner experiences, they frequently become more verbally articulate. Through the use of graphic or plastic expression, those who were originally blocked in speech often begin to verbalize in order to explain their art productions” (Naumburg 1987:1). Verbal contributions are equally important to the art therapist. It is vital to successful completion of treatment that the individual is not only picturing her unconscious but is able to verbally and consciously connect to its meaning as well. The following chapter describes a method I have developed to help the individual who is suffering from obesity or anorexia to identify the problem and manage its symptoms.
CHAPTER 4
Phenomenal and Nonphenomenal Body Image Tasks in the Treatment of Eating Disorders and Other Addictions (PNBIT): The Method
Art Therapy Session By the time a person suffering from an eating disorder presents himself at the art therapist’s office for treatment, he has identified himself as a failure. I have often worked with individuals who have reached a chronic stage and have been referred by a previous therapist or medical professional where there has been no, or limited, progress in treatment. This creates an urgent, crisislike environment. The client is apprehensive and resistent to treatment. It is important to establish the art therapist as a supportive educator, who accepts the person who is a patient but believes that patienthood is a transitory state. The harder but more urgent issue is how to engage the patient as one who believes in the value of art therapy. In addition to the problems of establishing trust, the therapist must be aware of the dual nature of addiction. It provides the affected individual with control of her life and, at the same time, creates constant fear of losing control. It is a rigid protocol. The challenge is to present the individual with tasks that require focus but also permit freedom within the framework of the art task. Each session requires that the person respond to the therapist’s request to produce a work that addresses a specific task. At the same time, using the materials offered, she is challenged to complete the project in any way she wishes. She is in charge of managing the —
27
—
28
— PNBIT: The Method
project—there is no control, but the need to engage her individual creative response to a problem. She is responsible for its completion and remains responsible, according to the permanent nature of art. Some art therapists will provide complete freedom in an art therapy session. The client is free to choose whatever materials in the room, i.e., pencil, tempera paint, crayons, watercolor, or oil, and any size paper that appeals to him. Sculptural materials and collage, i.e., fragments of printed matter, scraps of fabric of various colors and textures, small items that can be glued to a flat surface are also choices, among others. For some these may offer a receptive environment and be the proper approach. For those who are addictive, it may be too loose and too free. They would not be in treatment if they were not out of control. Therefore, it is my feeling that it is more useful to provide set tasks, within which the client is free. This provides a balance: freedom within a form; I call it safe haven. The Mandala work is especially useful, providing a predrawn 10-inch circle within which a client is free to respond in any way. The PNBIT is divided into two parts. The first consists of eleven individual art therapy sessions in which a task is presented to the client. The client completes one assigned task in each session. In the second half of the protocol the therapist presents the client with the same set of tasks, offered in the same sequence, with the same materials available. After completion of the two sets of tasks, the client compares the task from the first part with the same task from the second and comments on any changes she notes. The sessions are arranged so that there is ample time to complete each task. At each session the client is weighed, views herself in a full-length mirror and a hand-held mirror, and responds to the tasks on the Self Report Form (see appendix for a copy of the form). In addition, at each session the client is asked to respond to one body image art or expressive task in the order listed in the Sequence and Time Chart (see appendix 4 for a copy). The tasks are organized in descending order of structure, i.e., the first being the most and the last the least structured. After completion of the task, the client is asked to respond verbally to her rendering of the task. The therapist observes the process by which the client responds to the task and to the completed art production itself. These observations are reviewed with the client for any new meaning.
PNBIT: The Method — 29
Procedures, Materials, and Equipment Weight scale, full-length mirror, small hand-held mirror, cloth tape measure, tissue box, small box of crayons, red, yellow, blue, orange, green, purple, black, brown. Pad of white drawing paper, 14 by 17 inches, 10-inch circular template, 8½-by-11-inch white typing paper, tempera paints (come in small sets with basic colors), painting brush ½ inch wide, oil pastels (Craypas), No. 2 pencils with eraser. Assorted empty cardboard boxes, paste, scissors, magazines with pictures of people, furniture, scenery, food, drink, vehicles, houses, children, etc., clear plastic box, without cover, 11 by 14 by 2 inches deep (cover from a plastic picture box frame), sand to fill sandtray. Miniature toys (male and female figures, children and adults, domestic animals, dogs, cats, horses, cows, and exotic and wild animals. Abstract forms, broken items— mechanical or other. Stones, shells, seeds, etc. Two pounds of wet clay, base to work on, portfolio to store drawings, a place to store clay figures to dry, polaroid camera, audio tape recorder, a roll of white photography paper, 40 inches wide.
Phenomenal Tasks Weight Recording The individual is weighed without shoes at the outset of each session. The therapist and the client agree on the number of pounds the client weighs, while he remains on the scale. The client’s weight is recorded and dated on the Sequence and Time Chart, the Therapist Report, and entered by the client on the Self Report (see appendixes 2, 3, 4). Each client is weighed and compared with the recommended weight for height and body type. During this task the therapist is nonjudgmental and makes no comment on either weight gain or loss. If the client is engaged in a weight loss program, the details are not discussed unless a special problem relating to the client’s participation emerges. No dietary regimens are recommended by the therapist nor is weight gain or loss an issue during the course of treatment.
30
— PNBIT: The Method
Entries are dated and any comments by the client are noted by the therapist. The client is asked to respond to his weight level on the Self Report.
Mirror Viewing, Face The client is asked to view herself in a hand-held mirror at each session. The hand-held mirror is used to get a closeup view of features, eyes, hair, skin, and emotional state. The client records her reaction to these features on the Self Report.
Mirror Viewing, Full-Length The client is asked to view herself in a full-length mirror at each session, observing the fit style and colors of her clothing. She is asked to note any differences between inner feelings and outer appearance. Comments by the client are noted and dated by the therapist. The client is asked to view herself weekly at home, preferably undressed, in a fulllength mirror and record feelings in response to this exercise.
Body Dimension Estimates and Measurements (BDEM) As a preliminary exercise for this task, the client is asked to guess the length and width in inches of an ordinary tissue box and the resulting information is recorded. This is used as a basis for establishing the abililty of the client to estimate size (see appendix 23). . The client is presented with three figure drawings of the same sex as the client, ranging from anorexia to obesity. He is asked to select the figure which most closely represents his own current figure and enter it on the form (see appendixes 5 and 6). . The client is presented with two outline drawings of the human figure (same sex as the client): one for length (appendixes 7, 9) and another same-sex figure for roundness (appendixes 8, 10). Client is asked to estimate in inches the measurements of his linear dimensions, marking the estimates in the appropriate areas of the figure drawing marked “length.” This task is followed by a request that the client estimate
PNBIT: The Method — 31
the roundness of the various parts of his body and enter these on the second sheet, marked “roundness.” All the estimates are to be done without the aid of a measuring device. It is to be characterized as the client’s “best guess.” . In this task the therapist measures the same areas of the body estimated by the client, using a tape measure, and records the results in parentheses near the comparable estimates previously recorded by the client. Estimates and actual measurements are compared and discussed with the client. Implications are explored where the differences between the estimates and the measurements are more than 2 inches, either larger or smaller, or where the differences center on a particular area of the body. In this exercise the client experiences her actual body and is held accountable for any misconceptions. If the client doubts the accuracy of the therapist’s measurements, the part of the body in question is remeasured carefully, perhaps more than once, until the client is satisfied that it is indeed a true measurement. For individuals who suffer from eating disorders, distortion in body image may be exhibited by their inability to recognize their body size. Denial of body size permits continuation of inappropriate eating and feeding modes. The BDEM task helps the client bring to conscious awareness a more realistic appraisal of herself, a vital step in self-management (the drawing of the forms were adapted, based on templates one-eighth the size of female and male human figures). Prior to the first nonphenomenal task the client is presented with the Color Chart Form. The client is given a box of eight crayons and asked to use the colors, in any combination, to fill in the spaces of the circle. She is asked to write her response to each of the colors she has chosen in the spaces on the form. If the client responds to a color by naming an item of clothing or another physical thing, she is asked to expand on this by relating the color to her feeling about the color, e.g., “a good color, a sad color, a happy color, etc.” She is also to relate to the color in any other way she may wish; “blue reminds me of . . . ” These responses may be used later in treatment to identify positive or negative feelings in the later tasks. See appendix 22 for a sample form.
32
— PNBIT: The Method
Nonphenomenal Tasks Chromatic Family Line Drawing (CFLD) The client is given a box of eight crayons (Binney and Smith’s Crayola brand: red, yellow, blue, black, brown, purple, green, and orange) and a piece of 14-by-17-inch white drawing paper. The client is asked to make a picture of his family, using a crayon of his choice to represent each member. Each individual member is to be indicated with a stroke of the selected color. In this task the client is specifically asked to do the drawing by indicating, abstractly, the various members of his family unit. The client is then asked to sign, date and title the drawing (see figure 5.20 for a photograph of a sample CFLD). The following instructions are given to the client by the therapist: “On this sheet of paper, with these crayons, draw the members of your family. Draw each person not with a picture but with a line, using a color for each.” The CFLD, as the first nonphenomenal task, offers the client an opportunity to experience the art therapy situation with a simple project that can be completed in a relatively short period of time. This exercise also introduces the client to the therapist in a relationship that is continued throughout the project, i.e., the therapist is directing the session and, at the same time, the client is free, within the guidelines of the task, to respond creatively. The client is asked to label the family members with their names, near their place on the drawing, and to discuss his choice of color for each one. Any comments or observations by the client in response to observing the drawing are recorded by the therapist. The therapist responds to the client’s comments by asking questions about relationships and individual personality qualities of the family members. In this task the therapist is interested in the placement of the line that represents the client, i.e., where it is placed in relation to the other members of the family or if the client has omitted a line to represent himself. If the client has omitted her self-line, the therapist should make certain that the client has enough time and feels the task is complete. Of course, no direction is given to include the client. If, after giving the client
PNBIT: The Method — 33
the opportunity to change or add to the drawing, the self-line is still left out, this is discussed with the client during the general observation of the completed task. The CFLD does not commit the client to specific recognizable representations of members of her family and is therefore less threatening to produce. Nevertheless, the client illustrates her place in the family— indeed, tells the therapist whom she considers to be family—by whom she includes and where she places them in relation to each other. Inclusion or omission of the client, and his size, placement, and color in the scheme may indicate her feeling of isolation, special attachment, or alienation from the various members of the family. Under certain circumstances inclusion of family members or nonrelatives may be inappropriate and indicate dependency or fear and needs to be explored. Finally, the therapist discusses the drawing with the client as an art production. The choice of colors, the size of the lines in relation to each other, intensity, and placement on the paper are analyzed as a composition. This task is repeated after completion of the first rendering of the PNBIT unit and compared with the first CFLD for any changes. In evaluating a comparison of the first CFLD with the second CFLD, the outcome is considered to be positive if the client, who previously had omitted himself in the original drawing, spontaneously adds a place in the family for himself. Other favorable changes include the use of a different color for each person, inclusion of a member previously omitted, and placement on the page expressing realistic relationships in the family.
House/Tree/Person/Person (Opposite Sex)/Animal, Pencil (HTPPA/P) and Chromatic (HTPPA/C) The client is presented with a No. 2 pencil with an eraser attached and a sheet of 8½-by-11-inch white bond typing paper. The drawing of a house is requested, with the longer axis of the sheet placed horizontially before the client. Next, a drawing of a tree; after completion, a drawing of a person is requested, followed by the request for a drawing of a person of the opposite sex from the first. Each drawing is to be completed before the next is requested. For the drawings of the two persons and the tree, the longer axis of the paper is placed vertically before the
34
— PNBIT: The Method
client. For the animal, the axis of the sheet is positioned horizontally (as it was for the house drawing). Each drawing is made on an 8½-by-11-inch piece of paper. The client is asked to draw his “best” house and, later, his “best” tree and person(s). In the human figure drawing the client is asked to depict a whole person. For the drawing of the second human figure a request is made to draw a person of the opposite sex from the first drawing made. The animal, the last in the series, is requested by asking the client to draw any animal he wishes. In each of the drawings the client is timed and the time noted, but the client is allowed to take as much time as needed to complete each task. The client is permitted to use the back of the sheet to start again. Comments made by the client during the drawing task are recorded but are not responded to by the therapist. During the process of drawing the therapist is silent, except when specifically asked a question. Answers are kept as nondirective as possible. Nonverbally, the therapist encourages the client to focus on the task and to feel comfortable that any response made to the task is appropriate. The therapist is an active observer of the whole process: what part of the drawing was done first, last, changed, did the client turn the paper around from its original presentation, struggle more with one drawing or another, etc. Each drawing is signed, dated, and titled by the client at the time it is completed. After completion of the five pencil drawings, the client is asked a series of questions about each of the drawings starting with the last, the animal, and going back in order to the first, the house. The postdrawing interrogation is based on the guidelines suggested by Hammer (1958) and modified to keep the posttest interrogation less invasive to the client. Hammer’s original series did not include either the drawing of the person of the opposite sex or the animal. The following questions are posed to the client after completion of the pencil series, beginning with the last drawing and going back to the first. Answers are written down by the therapist. Animal 1. What kind of animal is that? 2. What sex is the animal?
PNBIT: The Method — 35
3. How old is the animal? 4. Is the animal in good health? 5. Where is the animal? 6. What is the animal doing? 7. Is that animal with other animals? 8. What kind of personality does the animal have? 9. Does the animal belong to anyone in particular? 10. What does the animal need? Person no. 2 (opposite sex from the first human figure) 1. What sex is that person? 2. How old is that person? 3. Is that person in good health? 4. What is that person doing? 5. What is the person thinking? 6. What is the best thing about this person? 7. What does this person need? 8. Could this person be someone you know? Person no. 1 1. What sex is this person? 2. How old is this person? 3. Is this person in good health? 4. What sort of person do you think this is? 5. What does this person need? 6. What is the best thing about this person? 7. If you could change one thing about this person, what might it be? 8. Does this person remind you of anyone? Tree 1. What kind of tree is this? 2. How old might this tree be? 3. Is the tree alive? 4. What time of year is it? The weather? 5. Which does that tree look more like to you, a man or a woman? 6. Is that a tree by itself, or is it in a group of trees? 7. Is this a particular tree?
36
— PNBIT: The Method
House 1. What is this house made of? 2. Is this house in good condition? 3. How old is this house? 4. How many stories does this house have? 5. Who lives in this house? 6. Where is this house? 7. Would you like to own this house? 8. Where might your room be? 9. Whom would you like to live with you in this house? 10. Is this house close by or far away as you look at it? 11. What is the weather like in this picture? After completion of the pencil drawings and the postdrawing inquiry, the client is offered a short rest period and a second set of drawings is requested. The pencil is removed and replaced with a box of Crayola crayons: red, yellow, blue, orange, green, purple, black and brown. Instruction for this series using the crayons is the same, i.e., to please draw her “best” house, except this time using the crayons. Parallel requests are given for the tree, person(s), and animal, all executed with the eight crayons presented. The client is given a fresh sheet of 8½-by-11-inch paper for each of the drawings. Paper is presented with the axis as in the pencil series, and general procedure followed as in the pencil drawings. The postdrawing inquiry uses the same series of questions as in the pencil protocol. The two series of drawings are produced in one session, allowing about two hours for completion. The series is repeated in treatment following the sequence as presented here. All answers and remarks made by the client are noted but not tape-recorded. As each drawing is completed, the client signs, dates, and titles them. For the client, the series of drawings becomes a historical record. The client is able to compare her responses at a distance in time from their making, when emotional reaction is modified by the opportunity to reflect on the material. This also gives a perspective on her overall body of work, factoring in the different responses to the tasks.
PNBIT: The Method — 37
The overall effect of the two series of drawings is that as a unit they serve as a miniature longitudinal study performed at two different time periods. Even though the pencil series and the chromatic series are administered close in time chronologically, they are separated in psychological time. The use of color taps into deeper layers of the personality. Projective drawing techniques are well documented as useful methods to assess personality. Machover (1949) said: In the production of a drawing there emerges out of the individual’s total experiential background a unique pattern of movement and idea, its significance for personality stems from the fact that there are involved processes of selection out of the infinite pool of experience and imagery potentially available in combination with a dynamic organization of movement and percept. . . . The individual who is directed to draw a person relates intimately to the impulses, anxieties, conflicts, and compensations characteristic of that individual. In some sense, the drawing is the person and the paper corresponds to the environment. (p. 5)
Mandalas Mandala (man´da-la), from the Sanskrit, means “circle,” in the ordinary sense of the word. As psychological phenomena, mandalas appear spontaneously in dreams, in certain stages of conflict, and in cases of schizophrenia. The severe patterning imposed by a circular image of this kind compensates for disorder and confusion of the psychic state through construction of a central point to which everything else is related or by a concentric arrangement of contradictory or irreconcilable elements. It may express either the totality of the individual in inner and outer experiences of the world or its essential point of reference (Jung 1959). Mandalas develop naturally in children’s art around two or three years of age. For this reason Mandalas, used with adults, may serve as a healing effect permitting symbolic regression to a time when the individual first experienced the Self as a total unity. The choice of a 10-inch circular template is also reminiscent of the view an infant has of the mother’s head appearing over the crib—a memory of a time of complete nurturing, both psychological and physical. Therefore the circle, provided
38
— PNBIT: The Method
by the therapist, offers a safe haven within which the client may feel free to work at the tasks. The client is presented with a predrawn, 10-inch circle, outlined in pencil on a 14-by-17-inch piece of white paper, and is asked to use the circle as a starting point for a picture or design in colors of her choice. Two Mandala tasks are assigned with the following focuses: 1. “Draw your body image” and 2. “Draw your self image.” Magic markers and craypas, pastels and tempera paints are made available as the media the client may choose to use. The first Mandala—the body image—is requested of the client following the session in which the HTPPA was produced. The second Mandala—the self image—is requested at the next session. After all the tasks in the protocol are completed, the two Mandalas are requested again at two sessions, one following the other. In the second series of Mandala tasks the client at times will assume more control over the assigned task, nonverbally, by going over the outline of the circle, freehand or by using the 10-inch template, and by choosing a more fluid medium or combining several. The Mandala helps the client visualize the source of polarities that have fostered some of her anxieties. Discussion and analysis of the individual Mandalas and especially comparison of the first and second version of the same task can be illuminating for the client. They permit her to see how her conflicts have been a function of her addictive behavior. See figures 5.15, 5.16, 5.22, 5.25 for examples.
Self Box (SB) The client is offered a selection of empty cardboard boxes, with and without covers, new and used, large and small, fragile and sturdy, round and flat. Other materials used for this task include current popular magazines containing many pictures, including scenery, people, food, houses, furniture, etc. Additional supplies include crayons, paste, and scissors. The client is directed to select one of the boxes to represent himself. He is asked to cut pictures from the magazines and design a collage on the inside and the outside of the box. The therapist describes the focus to the client: This task represents inner and outer aspects of yourself. Use the inside of the box to represent your private inner world, and the outside to represent yourself in interpersonal relationships in everyday encounters.
PNBIT: The Method — 39
The Self Box represents a many-sided portrait of the feelings, defenses, hopes, and fears of the client. The use of the box introduces a threedimensional quality to the art task and prepares the client for the sculptural tasks that are to follow. This task, as all the tasks, is to be administered in the sequence outlined, and repeated in the same order after the first series of tasks is complete. This task is adapted from Robbins and Sibley (1976).
Sandworlds (SW) The client is presented with a box of sand and miniatures of human figures, animals, building structures, vehicles, bridges, fences, stones, shells, and many other items collected by the therapist. The client is asked to make a selection from the collection of items that he wishes to use in the task. The therapist asks the client to take his selected items to the sandbox and build a scene, using the sandtray and any of the miniatures he has selected. He may return for more items or decide not to use all or part of his selections. When the scene is complete, the client discusses the items used in the SW and relates a story about them that is recorded in writing by the therapist. The story is then read back to the client, who may add or change any part previously narrated. Recurring themes that may appear are explored for meaning. The client is asked to title, sign, and date the SW. A color photograph is taken by the therapist to record it. Placement of the various items are noted by the therapist on the SW grid (see appendix 11 for a sample form). The use of miniatures to depict unconscious strivings may reduce self-consciousness, which sometimes limits expression in art media. Like the Mandala, the Sandworlds offers a built-in limitation, namely, the size of the box, offering the safety of set boundaries and, at the same time and within its limits, permitting freedom of expression to create a scene out of the client’s imagination. Kalff (1980), who revived interest in this technique, said, “For all true freedom, and thus also for the freedom of development, the sense of feeling sheltered is a prerequisite.”
40
— PNBIT: The Method
Kinetic Family Clay Sculpture (KFCS) The client is presented with a quantity of wet clay and a base to work on. The client is requested to make a sculpture depicting her memory of a family scene from her childhood and to place himself in the design. The sculpture presents a portrait of that memory and enables the client to symbolize her role in the family. This may represent a scene, positive or negative, that she may have previously thought about or visualized. The client describes the scene, how old she was when this occurred, and who was present. Analysis of the sculpture is for its aesthetic quality as well as illumination of the dynamics of her family patterns. This task complements the CFLD and brings into focus the client’s way of responding to family issues. The client signs, titles, and dates her sculpture. The therapist preserves the finished work for review and comparison with the second sculpture. When the therapist requests the client to repeat this task, during the second administration of the PNBIT, the client is asked to copy her original family clay sculpture, changing it to make it more positive— to improve its outcome. The two sculptures are compared and discussed with current feelings of the client about issues evoked and family members portrayed. In this exercise the client is allowed to regress symbolically while being cared for by the boundaries set by the structure within the task and the presence of the therapist. The invitation to change the outcome of the scene to a symbolically more acceptable one gives the client the power to change that which she felt powerless to do as a child. In the process, she may find that the outcome was inevitable, that she has now changed, or both. This task was adapted from Burns and Kaufman’s Kinetic Drawing Test (1972).
Combined Phenomenal and Nonphenomenal Task Body Contour Drawing (BCD) This task is initiated by the therapist who traces around the outside of the client’s body as he stands against a wall covered with a piece of white paper large enough to accommodate the client’s entire figure. The client selects the magic marker color, which is then used by the therapist to make the outline. The paper, taped to a wall, extends to the floor
PNBIT: The Method — 41
to allow room for the client’s feet. The client removes his shoes, and the therapist traces the feet as they appear on the paper. The feel of the marker going around the body assures the client that it is actually in touch with the reality of his physical body. If, after the outline is drawn, the client does not accept that the outline truthfully represents his body accurately, the client is invited to choose a second color. The therapist then proceeds to do a second tracing around the client’s body, using the second color selected by the client. The second tracing, in whole or in part as requested by the client, is slowly and carefully recorded over the first. The client is encouraged to have the therapist correct any part he feels is inaccurate and given every opportunity to change the outcome in a way that satisfies him: that it is a truthful rendering of his outline. Comparison of the two colors usually shows a remarkable similarity in the first and second tracings—often a surprise to the client. A full-length mirror is provided as an aid. The client is then directed to complete the picture by adding features, hair, and clothing. The client signs, dates, and titles the work. The client’s comments made during the process are noted by the therapist. After completing as much as possible, the client is asked to discuss the completed picture and these comments are taken down verbatim. The Body Contour Drawing Questionnaire is administered and dated by the therapist (see appendix 13b for the questionnaire). This task is repeated in sequence and compared with the first BCD for any changes in ability to complete the drawing. Changes in the client’s choice of color for the therapist to use in doing the second outline tracing as well as expressiveness and accuracy in depiction of the reality of the client are also noted. Analysis of this work is a sensitive process that may stir up powerful feelings and require several sessions of intensive work with the therapist to explore the production. The task puts the client in touch with the reality of her physical size. For the client who suffers from an eating disorder, either anorexia, obesity, or bulimia, this is an especially potent process. The slow process of looking carefully at herself in order to complete the drawing forces the client to face each of her physical qualities. Having to make decisions as to the items to include, emphasize, or change all play a role in helping the client acknowledge herself as a totality. The length,
42
— PNBIT: The Method
breadth, tactile quality, and, most of all, the client’s reality and aliveness are experienced nonverbally, over and over, and may help give credence to the idea that she exists in time and space. For these reasons the client may exhibit strong feelings when confronted with this image; for all its primitive execution, it holds a remarkable likeness to the individual portrayed. The BCD combines both phenomenal and nonphenomenal body image concepts in one task. The tracing fixes the client’s body as a bounded physical object in space. Ownership of the tracing is directly transferred to the client, who is then asked to complete it as a symbolic image through the process of drawing. The sequence of all the techniques in the PNBIT described above is administered in a gradual progression, starting from the most succinct and noninvasive task—the Chromatic Family Line Drawing—and culminating with the sensitive and provocative Body Contour Drawing. The progression of the tasks is designed to give the client a total exploration of her objective body dimensions and self-concept through both verbal and nonverbal modes. The opportunity to repeat the tasks and compare one with the other chronologically over time gives a unique perspective on the client’s progress. The client is engaged as an active participant in treatment. In clinical situations this therapist has found that the group of tasks works for both obese and anorectic clients, as well as for those with other addictive syndromes. An examination of the two series of drawings reveals striking differences. Even within a few months progress can be seen between the first and second renderings. Followed in sequence, the series is a powerful tool that can be used to move clients suffering from the effects of these stubborn syndromes toward healing and growth.
CHAPTER 5
PNBIT Clinical Applications
The PNBIT protocol has been developed over twenty years of clinical art psychotherapy treatment in a variety of settings: at Mount Sinai Hospital and Medical Center in New York and Phelps Memorial Hospital in Tarrytown, New York, among others. Populations included drug and alcohol as well as eating disorder addiction. A traditional research method was followed with each of a series of patients referred to the project from several facilities including Mount Sinai. An abstract of the study is in appendix 19 (Rabin 1987). Following are five case studies. Each describes the patient’s presenting problem as well as her progress. Before the start of the tasks the participants were given the Tennessee Self Concept Scale (TSCS), which was repeated at the conclusion of the second rendering of the tasks. The TSCS is a well-documented pencil and paper verbal measure of self-concept. A figure of each of the pre- and posttest results for the case studies is included. The data of the five case study reports presented are analyzed from the verbal perspectives of the Tennessee Self Concept Scale and the Self Reports. The nonverbal aspects are assessed through a comparison of the individual’s first and second renderings of the tasks. These evaluations are followed by a discussion of the meaning of these data and a summary of each. —
43
—
44
— Clinical Applications
In each of the case studies that follow, a woman embarks on a journey within the territory of the Self, much as the exploring infant first enters the frontiers of his physical being. Each participant became a pioneer, piercing the realm of that delicate boundary between the conscious and the unconscious, discovering in the process the mystery and order of the stranger called “myself.” I must have been four or five years old. I had been put to bed, kissed and tucked in; the light was out, but I was not yet asleep. As I lay quietly in the darkness an extraordinary thing happened: I was transfixed by the knowledge, the absolute certainty of my own existence. For the first time ever, apparently, I realized that I belonged body and soul to myself. When the shock of recognition passed, I seemed to wander about in my body, into my hands, up into my head, and down to the tips of my toes. I was intoxicated with pride, like a man strolling through some great estate which he had just inherited. “This is me,” I thought, “all me; and it’s been here all the time.” (Stevens 1983:140)
Megan Brown Tennessee Self Concept Scale (TSCS) Data Analysis
Megan Brown’s Total Positive Score (P) on pretest is 328, posttest it rises to 356. Her pretest P score is at the 25th percentile; her posttest result places her at the 60th percentile, a gain of 35 units. Megan’s Self Criticism Score (SC) is 38 pretest and 36 posttest— virtually no change and within normal limits for this item. Her TSCS profile shows gains in nine of the ten variables that measure positive scores. Notable in her increased posttest results are the variables of Identity, Self Satisfaction, Behavior, and Physical Self. Pretest, her Identity Score is 117; posttest, it rises to 123, a gain of 6 points, and an increase from the 15th to the 30th percentile. Self Satisfaction Score, 111 pretest, increases to 122 posttest. This represents a gain from the 68th to the 88th percentile. Megan’s Behavior Score, a low 100 pretest, increases to 111 posttest, indicating a change from a reading at the 8th percentile to the 35th, a gain of 27 percentile units. Megan’s entrance score on the item of Physical Self was practically nonexistent, a pretest reading in the 0.5th percentile. Posttest she gains 25 percentile units, a rise from a score of 51 to 67, a gain of 16 points for this item.
Clinical Applications — 45
Megan’s score for Total Variability decreases from 55 pretest to 46 posttest, a drop from the 72d percentile to the 42d percentile unit, a more favorable reading, indicating a less compartmentalized self-view. Her score for Distribution is 104 pretest and 110 posttest, a rise of 6 points and a change from the 23d percentile to the 30th, a rise of 7 percentile units, indicating a more secure feeling about herself. Megan’s Time Score pretest was seventeen minutes, posttest twelve minutes, both within normal parameters. In summary, Megan made gains in all but one of the items in the profile, and made significant gains in her overall P score. (For a comparison of Megan’s TSCS pretest and posttest results, see figure 5.1.) Megan learned of this project through a notice in her university student newspaper seeking subjects. At the screening interview Megan stated that she wished to participate in the study because “I want to become more comfortable with myself and particularly with the female part of myself. I’m a pretty good human being, but I’m a lousy woman-female.” Megan is 5-feet-3½-inches tall, has a small body frame, and weighed 180 pounds at entrance to the program. According to the Metropolitan Life Insurance weight tables (1983), she was 60 pounds over the recommended weight for her height and body frame. Megan is a twenty-five-year-old white woman, with dark hair, brown eyes (her most appealing feature), and a smile that she showed often but not always authentically. She is articulate and intelligent, studying for a professional degree. At the initial sessions, she wore large-scale, heavy, horn-rimmed eyeglasses that covered most of her face. Her hair was cut blunt and short, and it also masked her face. Two striking features were a number of prominent, raw, red pimples on her face and hair growth on her chin, which she unsuccessfully tried to cover with makeup. She wore ill-fitting, bright blue pants, a poor substitute for “jeans.” Out of keeping was a prim blouse with a lace collar, and over all, a too-large black coat that enveloped her like a shroud. The general effect was discordant and lacked integration. . Megan is a student in a large university where she is studying for a professional degree and expects to graduate in a year. She is single. She was born in Europe and, as a result of her father’s military
Raw Scores
117
123
111 122
100 111
51 67
76 80
63 66
69 68
75
69
46
55
25
28
21
27
104 110
Pretest Posttest
T —95 — — — — —90 — — — — —85 — — — — —80 — — — — —75 — — — — —70 — — — — —65 — — — — —60 — — — — —55 — — — — —50 — — — — —45 — — — — —40 — — — — —35 — — — — —30 — — — — —25 — — — — —20 — — — — —15 — — — — —10 — — — — —5
by permission of the publisher, Western Psychological Services, 12031 Wilshire Boulevard, Los Angeles, CA 90025.
Answer-Profile Sheet (W-182B) copyright © 1964 by William H. Fitts. Reprinted from the Tennessee Self Concept Scale
Megan Brown: Comparison of Results of First and Second Tennessee Self Concept Scale
356
—
328
38
0.01
MEGAN BROWN
0.01
36
0.1
1
0.1
5
5
1
10
10
Tennessee Self Concept Scale Pretest (17 Min.) Posttest (12 Min.)
20
20
Percentile
70 60 50 40 30
D
80
Row Total V
70 60 50 40 30
Column Total V
80
Total V
VARIABILITY
95 90
Column E Social Self
95 90
Column B Column C Column A MoralPersonal Column D Physical Self Ethical Self Self Family Self
99
Row 3 Behavior
POSITIVE SCORES
99
Row 2 Self Satisfaction
99.9
Row 1 Identity
99.99
Total Positive
99.9
Self Criticism
99.99
Percentile
Figure 5.1
95— — — — — 90— — — — — 85— — — — — 80— — — — — 75— — — — — 70— — — — — 65— — — — — 60— — — — — 55— — — — — 50— — — — — 45— — — — — 40— — — — — 35— — — — — 30— — — — — 25— — — — — 20— — — — — 15— — — — — 10— — — — — 5—
T
Clinical Applications — 47
service, has lived in many locations in the United States since she was two and a half years old. Though she will be enabled to earn a high salary when she is finished with her studies, she was resentful and unhappy, feeling that her parents had pushed her into her choice of career. She stated that she would prefer to own a restaurant and was seriously considering dropping out of school. She works part-time, her parents contributing very little of the money needed to pay for her tuition; mostly Megan has had to borrow money through student loans and, as a result, is heavily in debt. . Megan states that she “always had a weight problem” as long as she can remember. As an adolescent she weighed approximately 140–150 pounds, in college 140–160. In a report to the therapist her physician writes that she was diagnosed as moderately obese when she weighed 157 pounds. Since that time she has gained 22 pounds. Megan was conscious of her weight as early as five years of age, when her father served in Vietnam. At that time she gained 20 pounds in one year, the result, she feels, of separation from her father, whom she regarded as her protector (from her mother who abused her). In the past she attended Weight Watchers where she “lost 20 pounds three times.” Megan discusses her feelings about fat people: “I think fat people are weak, self-indulgent, and have no discipline. All things I also think about myself.” Megan describes her eating problem: “[I] tend to overeat on a daily basis . . . like sweets . . . and overeat dessert at every meal. . . . [I] ate a whole Carvel cake. I eat too much, frequently in stressful situations, but I also eat to celebrate, too.” She had not been in treatment for psychological adjustment problems before entering this program, although she had one session with a psychologist the year before joining the project. . Megan was delivered in a hospital and weighed 7 pounds 8 ounces. At six years of age she suffered from migraine headaches (a medical report by her physician notes two to three headaches weekly). Megan reports that at two and a half years she was “three seconds from drowning,” she had “pneumonia at twelve,” and described herself at fourteen as “suicidal” due to depression. The only childhood disease reported is chicken pox; at seventeen she had surgery to remove a ganglionic cyst from her left wrist. She reports that she has difficulty distinguishing left from right and therefore has difficulty driving a car. Her doctor reported
48
— Clinical Applications
unilateral bruising, but the source was not identified, and several episodes of what appeared to be food poisoning were also noted in the medical report. She reported having used drugs “at one time.” She complained of back pains, which her doctor thought may have been due to her weight. At the time of the project she was being treated for an eye muscle problem and was receiving training to correct this condition. It had seriously interfered with her ability to sustain even moderate periods of reading for her studies. . This is the first marriage for both parents. Her mother is forty-six years old, suffers from varicose veins, and is slim. Her mother returned to school at forty, earning a professional degree in the same field in which Megan is studying. Her father, forty-eight years old, is a professional scientist. He is 6 feet 2 inches and weighs 200 pounds. Megan reports that he is overweight, has a back problem, and suffers from a persistent rash and sores because of exposure to Agent Orange in Vietnam. He is unemployed. Megan feels he could work but is passive and is not trying to get a job. He allows his wife to make important family decisions. Megan has one sister, one year younger than herself, who is 5-feet6-inches tall and weighs 110 pounds. She suffers from allergies and is also studying for a professional degree, but different from the one that Megan is preparing for. Megan reports she has always had a good relationship with her sister, but recognizes that her sister was spared the brunt of problems at home. She said, “My mother has been beating me down (emotionally) since I was a child.” In a follow-up session after completing the project, she relates an incident on a return visit to the family. Her sister reminded her and the parents of a time when her mother beat Megan physically. Megan was amazed that she had blocked out the physical abuse and only remembered the emotional. She observes, becoming consciously aware for the first time, “I was the one who got the shit beaten out of me!” Project Compliance
From the outset Megan was committed to participating in the study. She was reliable about keeping appointments and cooperative
Clinical Applications — 49
during the sessions. There were sessions she found painful, and there were many tears. She never wavered in her determination to complete all of the tasks. At the end of the project she writes, “This is the most significant thing I have ever done. Period.” Repetition of the tasks was useful for Megan, and this was echoed by several of the other subjects. Although many of the tasks were nonverbal, Megan found it necessary to talk a great deal prior to beginning each task, perhaps as a resistance. She was compulsive about telling the therapist everything she had thought about between sessions. She often made notes during the sessions so that she would not forget to tell the therapist all her thoughts. As Megan became more confident in doing the tasks and less fearful of what would emerge, she was able to defer her need to talk and get to the task at hand more easily. Her initial rendering of the House/Tree/Person/ Person/Animal task took her two hours and twenty-five minutes, but the second HTPPA series was reduced to one hour and forty-nine minutes. Her ability to delay satisfaction was a signal that she was better able to deal with stress on her own. Her intelligence and ability to gain insight to the dynamics made the work move quickly—perhaps too quickly, as she did not allow herself time to assimilate the material. At one point near the end of the school semester she accepted a summer position in another state and would leave the city for three months. She agreed to come more often so that the tasks would be completed before she left. This increased the intensity of the sessions. While she was willing to participate in this telescopic manner, it became apparent that it would be difficult to deal with some of the issues, and the time between sessions was increased again. During the course of the project Megan’s health was reasonably good, although she did report migraine headaches and one cold. Megan completed the tasks in twenty-three sessions and spent about sixty-five hours doing the tasks. Contact was maintained by mail and telephone until she returned in the fall, when she was seen in follow-up. The therapist recommended that Megan consider entering therapy in order to stabilize her gains. She has since made contact with a therapist near her school and is feeling comfortable with this arrangement.
50
— Clinical Applications
Phenomenal Tasks
. Megan voluntarily began attending Weight Watchers soon after starting the project, but, after losing seven pounds, she discontinued attendance. She had no difficulty in recording her weekly weight in the sessions. , . Viewing herself in the face mirror was very difficult for Megan. She was anguished by the presence of the facial hair. Her gynecologist diagnosed the hair growth as a hormonal dysfunction. While the growth might be slowed or stopped by treatment, the hair already visible would not be eliminated. Electrolysis was the only permanent way to remove the hair growth. The facial hair created enormous feelings of disgust within Megan, and undoubtedly it was also a considerable deterrent to social opportunities. Her parents had agreed to pay for removal of the hair by means of electrolysis, but not until Megan graduated from school, which was still eighteen months away. Options for solutions to this problem were explored with the therapist. Megan borrowed the money for this purpose from her grandmother and immediately began corrective treatment, which continued throughout her participation in the project. Though she moved to another city for her summer job, she continued in treatment and the condition improved. This action by which she assumed responsibility for her own care was a step toward recognition of her emerging independence from her parents and both her ability and need to make decisions for herself in an appropriate and mature manner. There were other such experiences, such as shopping for clothes for herself for the first time. Since she was two, her father had shopped for Megan’s clothing; his decisions controlled how she would look to herself and others. Later, when her great-grandmother died in a nursing home, Megan was given all her clothing. Megan was wearing her great-grandmother’s clothing and shoes when she first came to participate in the study, justifying it because they were of “good quality.” Gradually, she gave up wearing these items as she purchased and began wearing new ones. At the end of the project her outer appearance had changed dramatically. She had gotten a new hairstyle, contact lenses replaced her horn-rimmed eye-
Clinical Applications — 51
glasses, and she was wearing facial and eye makeup, perfume, earrings, and dresses, instead of the ill-fitting pants, and her own coat and shoes. She felt like an emerging butterfly, saying, “My eyes look like butterflies,” and delighted in it. In her drawings—especially in the Mandalas—we see these elements depicted. Butterflies, flowers, and gentle sunsets and soft colors abound. Catching her reflection in the mirror, she asks, “Who is this attractive adult woman?” , -. Megan began to accept herself, and reported enjoying caring for herself, removing her makeup at night, and touching her face with care and gentleness, things that were new for her. She tried to “see what and who is there.” At one time she reported looking at herself in the mirror and seeing her mother reflected. Frightened by this, she worked at concentrating to restore and hold constant her own image. Other times she found the image in the mirror changing, “starting to look larger as we sit here.” Finally, near the end of the study, she reports with relief and joy: “Every night this week, my body seemed stable in the mirror.” As she experiences these changes within herself, she reflects on her family situation and recognizes that her “mother was made to be the heavy in the family.” ₍₎. Megan was not able to estimate her roundness accurately; in general, her estimates were almost twice as small as they actually were. Nevertheless, she accurately estimates her thighs, which were an area always focused on negatively by her mother. Megan estimates the circumference of her head to be only 13 inches when it actually is 22 inches. Perhaps this reflects the feeling that although she knows on one level she is intelligent, self-devaluation makes her feel less able. She acknowledges, “constant low self-esteem (because I’m overweight, have small breasts, and a lot of facial hair). I think I’m afraid of ego out of control, of playing too many games, of men, of being promiscuous.” She begins to become aware of what she is eating, how much, and whether she wants to eat, becoming more conscious of her physical needs.
52
— Clinical Applications
Nonphenomenal Tasks
₍₎. In her first CFLD Megan uses multiple colors for each member of the family, a somewhat unusual response to the task. She assigns black and red for herself, a reflection of active and passive strong feelings, both anger and depression. Her father is depicted in black, brown, and blue, her mother blue, orange, and green, and her sister yellow and green. The mother shares the color green with the sister and the father shares red with Megan. Megan positions herself as the family member farthest removed. Although she shares the red color with her father, she puts herself at the greatest distance from him, acknowledging the conflict of her dependency and need to separate. Although she is closer to her sister than she is to her parents, she gives her sister a higher position than herself, reflecting Megan’s feeling that her sister is “better” than she is. In the second rendering of the CFLD Megan increases the number of colors assigned to each member: her parents and her sister gaining one additional color. Megan gains three, an acknowledgment of her increased understanding of herself in relation to the family. She labels both the first and second drawings in purple, her own individual color. She notes at the final session, “The colors are coexisting.” Notable in the second drawing is the removal of the black color from her own line, though the red remains and is still shared with the father. She is no longer depressed about herself, but issues remain to be worked out with her father and mother. She does not share her mother’s orange color. She writes, “Daddy’s little girl—being thin or dependent will not make you his little girl. He has to grow up to where you are.” ⁄ ⁄ ⁄ ⁄ ₍₎. The first chromatic tree drawing is that of a Japanese bonsai, heavily crayoned in black and red. Megan labels it “Stunted Bonsai Tree,” spending eighteen minutes doing this drawing. She became depressed after doing this drawing and needed to return to it during several subsequent sessions. She describes this tree as being five hundred years old, in a sunset by itself, looking more like a woman than a man. Of the bonsai, she says: “They are beautiful but disturbing and unnatural, purposely stunted by people.” She makes the connection to herself. She is shocked and says: “It’s my colors! Bonsai doesn’t
Clinical Applications — 53
let trees be trees. Ties into my feelings about women—they are badges of the fact that bonsai trees are feminine trees grown by men.” She feels the tree is ready to be transplanted as it has outgrown its pot (see the first drawing of figure 5.2.) She expresses feelings about herself. She has, like the bonsai, been kept in a pot by her father, who restricted her development and growth. Through his passivity and lack of awareness that she had outgrown her pot, she was neglected, unnurtured. Her anger toward her mother, who should have been the nurturer, is evident. Her mother, for reasons Megan now better understands, delegated her care to others, abdicating the mother role to the father and grandmothers. Megan’s chromatic tree drawing in the second series is a dramatic change from the first. The second tree is essentially the same shape as the first, but it is now outside, transplanted, alive, and growing. Megan titles the second drawing “The Tree on a Hill at Sunset in Color.” The picture is strong, but the application of the colors is less pressured. There are many new colors—including green, purple, brown, orange, yellow, blue. Of her old colors the red here is used only minimally to increase the intensity of the sun, and black appears diluted as gray on the trunk. The colors are gentled and the tree has lost the barblike branches that were a feature of the drawing of the bonsai tree. The tree is given support by a groundline and centered between two breastlike hills, symbolic of the mother, but it stands solidly on its own. Megan says this tree is twenty-five to thirty years old, close to her own age, and that it is summer; the tree is among other trees (see figure 5.2 for a comparison of Megan’s first and second chromatic tree drawings.) In the first HTPPA series Megan’s chromatic figure drawings are rigid and incomplete, presenting an immobilized robotlike stance. Static and contained and drawn in profile, the first HTPPA series female figure has a warlike aspect. No features appear on the faces of either the male or female figures, and no hands or feet. Though the female has a dress, no other sexual identity is apparent. The deep orange skin of the face, arms, and legs of the female figure may reflect her own identification with her father’s exposure to Agent Orange. The first chromatic female figure is done in black and red, Megan’s early colors, unmistakably representing herself. Of this drawing Megan says, “Softening the shoulders would be one thing to change about this person.”
54
— Clinical Applications
Figure 5.2
—
Megan Brown: Chromatic Tree from HTPPA Comparison of first (top) and second (bottom)
Clinical Applications — 55
Figure 5.3
—
Megan Brown: Chromatic Female Figure from HTPPA Comparison of first (left) and second (right)
In the second series her female figure becomes a softer, more humanized person, certainly female, graphically depicting a growing sense of her sexuality and identity. (See figure 5.3 for a comparison of Megan’s first and second chromatic female figures.) In summary, Megan’s HTPPA prognosis is good but guarded. Megan’s first series drawn tree is better than the drawn person. Though she calls it a “Stunted Bonsai Tree,” it has all its parts. She says of this, “It has outgrown its pot, it is ready to be transplanted.” Indeed, in the second series the little tree is seen transplanted in both the pencil and the chromatic house drawings. It is a sign of growth and potential. In the figure drawings there is dramatic improvement from the first to the second series.
56
— Clinical Applications
The first female figure drawing (as well as the male) is rigid and immobilized, it has no hands or feet and is seen in profile without features. This is a desexualized portrait and an accurate graphic depiction of her feelings about herself at the time it was made. She reconciles this in the second series, transforming robotic figures into sexually recognizable human beings. In the second HTPPA the pencil and chromatic are closely related in their psychological quality, and, though significant gains were made, it was felt that to stabilize these further therapy should be undertaken. The therapist recommended to Megan that she continue in therapy if possible at the completion of the study. ₍₎. Megan’s first Self Image Mandala is a series of three disconnected designs composed of tiny dots, hearts, and lines, none of which is complete. In the center of the Mandala is a heavily colored square shape in black with red concentric lines and bands within it. In the center of the black square is a tear in the drawing Megan made when coloring it. She compulsively and repeatedly went over the center with a yellow magic marker and eventually wore a hole in the paper. (Yellow is her sister’s color in the CFLD.) Of the first Self Image, Megan says: I wanted it to be busy; dots make it complicated. I drew a black line around the whole thing. I wonder, if I change all the externals, will the inside stay the same? I don’t always want to be a fat person on the inside. I want to be a normal average weight; the person in the inside. I don’t want it to be a charade. The part in the middle, I didn’t want it to touch the other parts. Three parts: physical, emotional and intellectual. I wanted to keep the dots in control. What am I going to put in the other spaces? I couldn’t think of anything.
Of the yellow, she says: I wanted it to be like a sunny day, with a lot of yellow in it. . . . I felt very funny putting the yellow in the middle and was very upset when it (the color) ran—but that’s where the yellow belongs. If you don’t like the yellow you can cover it up with the black. When the black ran into it, I realized that it really belonged there.
Here she asserts both her place (the black) and her sister’s place (the yellow): that both have to coexist.
Clinical Applications — 57
Megan’s second Self Image Mandala, titled, “Self Image in Disjoint,” is a more complete composition; the background is softly colored in blue, sprinkled here and there with golden stars. In the upper right-hand section is a mandalalike sun. On the opposite side is a bouquet of flowers and, in the lower third, a lace-stockinged leg is in a kicking position. She analyzes this Self Image: Stars are magic potential: “Reach for the stars.” A mandala within a mandala—fusion. Inside connects to the outside; flowers, discovery of the feminine aspect. The leg is the sexual side (bad girl colors): disjointed, uncomfortable feeling in relation to sex and how to integrate that into the rest of my life. Three things are moving closer to each other.
Megan’s first Body Image Mandala is a target design. It has a black and pink center. She says of it: An image of hell. If I lose weight, my whole life is going to change. Interaction with people will change—that’s scary. Femaleness means going out of control. The black and blue and pink mandala is poisonous and futile and capable of getting out of control. I don’t measure up to what a pretty girl should be, and therefore heaven forbid I should be sexual. Some of it comes from me and some of it comes from other people.
The second Body Image Mandala, done six weeks after the first, depicts a series of items divided into four quadrants. In the upper left eyes made up with a realistic rendering of her eye makeup. Upper right: a purple butterfly. Lower right: a section of the night sky, a yellow half-moon, and ten stars. Lower left: a pink, blue, and green exotic flower. The inside background is light blue. The outside of the Mandala is ringed in a border of yellow and red tulips; green stems connect the whole. One purple tulip appears in the ring; outside the circle in the lower left-hand corner of the paper is a set of soft pink lips. She calls this Mandala “The Body in Progress.” Of this drawing Megan says: A lot going on—things had to go on the outside because there wasn’t enough room on the inside. There’s a lot of layering. Things have not shifted totally into place yet. Takes time to penetrate to the inside. I had planned to put the lips on the inside. The circle wasn’t as big as I thought it was. Blue is a protective coating, like a bandage. Moon and stars: body
58
— Clinical Applications
tied up by the tides. The moon is not complete yet. Eyes: part of the body I’ve been focusing on, makeup, contacts. Eyes are calmer, but still . . . hesitant. Blue and red orchids equal feminine. Butterfly is the metamorphic quality: “Here I am!” Physically standing there. The flowers on the outside: discover the inside through the outside. One purple tulip—I love purple tulips—doesn’t always have to be the same.
Megan notes that the second Body Image Mandala is more balanced. The Mandalas evoke memories of her three grandmothers. She says: My great-grandmother died thin last year. She was in a nursing home. They gave me her old clothes and I have been wearing them. My greatgrandmother was always thin, always fragile, died between ninety-four and ninety-five. My other great-grandmother was always hearty. She made a choice to die instead of going into a nursing home. She refused procedures and died of pneumonia. She was in control until the end.
Now she suddenly makes a connection: “My [other] grandmother bought jeans too big for me. I was eating to fill them up!” Megan compares the two Body Image Mandalas: “I really don’t like looking at the first Body Image Mandala. It’s like an old ghost, because I haven’t completely rid myself of all the things that are going on. I’m not completely free.” Later, comparing all four images, she gets a perspective and says: I feel a lot less bitter. The backgrounds of the two later pictures are softer. Evenness. I haven’t been depressed in months. I was bitter about men. I feel much better about myself. I don’t have an axe to grind with them anymore. I don’t know how it came about. The early pictures are abstract. The top has representational things, getting in touch with physical qualities, confronting the mirror.
₍₎. Megan’s first SB, called “Self in a Box,” is a cubelike shape, much like her early figure drawings, static and incomplete. It is devoid of color on the outside except for a broken cup on the top. No natural human figures appear on the outside. Two male marble statues are pasted on one side. They each have long, flowing beards. Inside there is a butterfly, a pair of pink knitted baby booties, loose pearls, and a woman’s head. Three caricatures of devils with horns and tails are actively talking. One holds a
Clinical Applications — 59
pitchfork. Pasted on the top of the outside of the box are the words “Is it a boy or a girl?” The second SB is called “Arapacis, the Altar of Peace.” This box is round, and she carefully covers it with white paper on which she pastes the collage. She says, “This time it’s most like a human form. All the others were squarelike boxes. This time I needed and wanted less things.” On the outside she has chosen a face of a pretty woman with a butterfly on her head. Her chin is wrapped in blue gauze. In her second Body Image she makes reference to the color blue as a “protective coating, like a bandage.” The removal of the hair on her chin and the nurturing quality of that process are embodied in this picture. The male statues are gone and in their place appears a standing marble statue of a female figure holding the hand of a small child. There is a large bouquet of flowers. Inside this box the knitted baby socks are replaced with a high-heeled woman’s shoe, a sensuous, seated woman, back toward the viewer, is nearby, and also a female hand holding a bottle of perfume. The top of the box is loosely fitted, allowing the inner and outer a more open and continuous relationship. There is less compulsion to include everything. In each of the tasks Megan gets a little closer to totality. She is still struggling to reconcile her masculine and feminine aspects. She is beginning to grasp that she will have to make some choices. In her search for both freedom and security she finds that, though they may not always be compatible, they are complementary, and both are needed to complete the circle. More time is needed for her to take hold of the means to achieve this idea. ₍₎. Megan’s first SW contained twenty-three items, the second only fifteen. She says, “This is enough.” The first SW is titled “Double Image.” She makes an imprint of her right hand in the center of the sandbox. Megan analyzes the process: This was very different than the first. Artificiality had meaning before. The second time should be fresh and original. Last time was overintellectualized, and this time as I picked pieces I became aware that I was picking double images. Three-quarters of the way through I realized the meaning. I wanted to do a circle . . . didn’t want anything inside the hands. Inside the circle are immemorial things—timeless. The watch: time, light:
60
— Clinical Applications
candelabra (elegance). Seashell: tides, ocean, water, harp: music (forever), white horse: Cinderella, “Sometime my prince will come.” Came out of the past, has some armor on. On the outside of the circle everything is doubles. Interesting the way I positioned the ballerina—shepherd, female-female doubles not facing. Gazelles, graceful, and turtles—are they looking in and out? Female in and out back to back. Turtles and gazelles are facing each other. The lens is a tribute to seeing whatever there is about it. Turtles are mirror images and the ballerinas are mirror images. Tribute to the mirror! I’m thinking I’d really like to have a boyfriend!
(See figure 5.4 for a photograph of Megan’s second SW.) An important theme emerges in this exercise: Megan’s recognition of her sexuality and her identity. This is a recurring theme appearing in her work that asserts itself both for the viewer and on the part of the creator, which underlines its authenticity. ₍₎. This was one of the most significant tasks for Megan. Her first response, titled “The Camping Family,” depicts her memory of a family outing when she was nine or ten years old. Though
Figure 5.4
—
Megan Brown: Sandworlds Second scene, closeup
Clinical Applications — 61
Figure 5.5
—
Megan Brown: Kinetic Family Clay Sculptures Second scene
she describes this as a good memory, after analyzing it she acknowledges that the memory was a distortion of reality. In the first scene the family members are separated from each other. In doing the sculpture a second time, in response to the task to “make it better,” Megan recreates the images and assembles the figures, seating them close together on a log. It is difficult for Megan to face this scene. She says, “[The KFCS] allowed me to see what makes me so very sad about my family (and I guess about myself, too). . . . The sculpture . . . said to me, ‘salvage what was good out of what was to improve your own what is.” (See figure 5.5 for a photograph of Megan’s second Kinetic Family Clay Sculpture, which she titles “The Foundation”). Combined Phenomenal and Nonphenomenal Task
₍₎. Her first BCD shows an empty, transparent body with an inappropriate red heart spewing stars within the body. The hair, horseshoe-shaped, rings the head in a bilious green. The hands are two colors, one yellow and the other orange. The rest of the body is undifferentiated, empty, and grotesque; it is undressed except for socks. The
62
— Clinical Applications
body boundary is broken and poorly defined. In her second BCD, done five weeks later, her gains can be seen in her use of softer and more natural colors and in her completion of features and clothing in a realistic manner. The body boundaries are clearly marked, giving the figure substance. (See figure 5.6 for a comparison of Megan’s first and second Body Contour Drawings).
Figure 5.6
—
Megan Brown: Body Contour Drawing Comparison of first (left) and second (right)
Clinical Applications — 63
Self Report
. This is an excerpt from a tape recording made after Megan’s first contour drawing. When I look at the figure in the mirror and I look at the figure on paper, the figure on paper is more real. The figure has more psychological reality for me because I colored it in, and when I look in the mirror . . . it’s kinda hard to explain, but psychologically I don’t know what I’m seeing and physically I don’t know what I’m seeing. Now when I look at this piece of paper . . . now physically I’m not just sitting there . . . within the session it keeps changing . . . smaller than I thought it would be . . . now expanding to fill up the proper amount of space it needs. But it has a much greater psychological reality for me than what I see in the mirror. . . . Anorectics see their bodies as things—now that’s exactly how I see my body. . . . What a horrible way—I think of myself as a prisoner of these thighs—a prisoner of these hips—of this stomach. What a horrible way to think about your own body—as a prisoner of your own body. One of the things I’m really struggling with is that you are a composite makeup of the mind and the body. You are both those things—and if I think that inside that I’m beautiful and I kind of think that I am, what the world sees is not my inside and I don’t think that anybody ever sees your inside, they can’t. . . . If I think that the inside is beautiful, why have I been not letting the outside be beautiful for such a long time? It’s not such a bad outline. I think of all the times I looked at the mirror and hated my body. I never want to feel that way again. I tried it this morning, looking in the mirror and saying “I love this body,” and I can’t do it—not yet. At least I’m looking. I don’t have the nausea that I had looking in the mirror before. Repetition has helped in and of itself. The first time you had me stand there and had me look in the mirror . . . I don’t know how long it was . . . but thirty seconds felt like five minutes. At times now I’m looking forward to putting on my makeup. I feel really solid about these things . . . very solid. But I suppose there’s always the fear, like a drug addict or an alcoholic, and have a relapse; I’ve dealt with them [problems]. I haven’t urges to abuse myself. I caught my image in the mirror and I thought I looked pretty nice and kept walking. I have actually been nice to myself in certain ways. Yes, I bought myself some flowers.
64
— Clinical Applications
Later Megan compares her first BCD with the second BCD made five weeks after the first: The first contour of the body is much more of a psychological drawing. I like the first one on a color level, but on a psychological level it’s a little scary, there’s a zombielike element. First . . . I drew the heart to be . . . sort of a loving element, but it really isn’t, it really is an explosive element . . . only other indication of a person is in the face. Even the hair is only a horseshoe. [In the second BCD] there is much more contact here with physical realities in terms of clothes, jewelry, nail polish—even the face. There are few colors used in appropriate places; this one is more of a physical portrait, more realistic, physically more attractive. . . . The hands match, this time. I’m a little calmer about myself—I’m not particularly afraid. I’m almost trying to enjoy looking in the mirror and enjoying my body. I only got me. The eyes are bigger in the space, letting the irises have as much space as they need. The face is calmer, lips are not bright red. I’m nervous about saying the first one is no longer an accurate depiction of myself. Progress: both are afraid, but one is more relaxed afraid. This is the first time in my life I’ve ever said “I’m afraid.” I was never allowed to be afraid. My father was not allowed to be afraid. I was not aware that I was afraid. I’m tired of not being aware of certain things. I can give myself confidence and let my colors show . . . to be calm and let myself be lovely. . . . There’s a softening thing that’s going on in my voice—it’s almost a whole human being.
. See table 5.1 for a comparison of Megan’s answers to a series of questions on her first and second Eating Questionnaire. Discussion
Megan is in conflict in relation to her need to separate from her family, reflecting issues of power and dependency, a pull between growing up and remaining dependent for the security she needs. She yo-yos back and forth between separating and returning, as if her weight gain and loss are a reflection of this process, ingesting and purging herself. This is also connected to the conflict between the parents. The mother has assumed the authority of the breadwinner, and the father reverses roles with her. Megan is caught in this dilemma. Because her mother had
Clinical Applications — 65
Table 5.1
—
Megan Brown: Comparison of Responses to Eating Questionnaire
Question
Answer 1
Answer 2
Do you consider yourself to be a fat person? Why, why not?
No. I am overweight— big thighs, big hips, big stomach.
Yes and no. I now consider myself an overweight person, i.e., a person with a weight problem, but one that is under control and can be managed.
Do you consider yourself to be attractive? In what way?
No. Too heavy, small breasts, big thighs, bad skin, too much facial hair.
Yes and no. I have nice clothes, which I’m beginning to combine in more feminine and flattering ways. I look more and more like I’m taking good care of myself—that I’m well kept (by myself).
What is your best asset?
Good sense of humor, sharp mind.
On a physical level, my eyes and my smile. On a nonphysical level, I suppose my best assets are compassion and sensitivity (secondary: intelligence, a sense of humor).
Whom do you blame for being fat?
No one. Maybe myself, maybe my mother.
I suppose for a long time I blamed my mother and myself. Now I don’t really pin the blame on anyone.
Why?
My mother has been beating me down (emotionally) since I was a child.
There is no blame, just a combination of unhappy circumstances and distortions.
Are you proud of your achievements?
No (not most of them anyway).
Yes.
Which ones?
No answer.
Therapy, some photographs I have taken, a clay duck I once sculpted. My upcoming job (maybe).
Why?
I don’t give myself credit. If I can obtain it, it must not be a big deal. I wouldn’t belong to any country club that would have me.
Photos and duck are manifestations of my nonintellectual self.
(continued)
66
— Clinical Applications
Table 5.1 (continued) Question
Answer 1
Answer 2
What do you believe to be the cause of your eating problem?
No answer.
Inadequate self-esteem (and a great deal of disconnection about what was upsetting/troubling me and why and when).
What goal in your life would you like to achieve?
I would like to own a restaurant. I want to have children.
I would like to get married and have children and remain sensitive to my family’s needs and to teach my children to recognize their own needs and deal with them (self ministration)
never been the nurturer, Megan’s sexuality was at risk. Megan sought this nurturing elsewhere and found numerous surrogate mothers to substitute for this missing link as well as, finally, food. Her great-grandmother was such a figure in her life. Wearing her dead great-grandmother’s clothing was an attempt to resurrect the warmth of the encasing container. Walking around in the great-grandmother’s clothing created the bizarre illusion that she was still alive. It became a grisly daily rite of denial that the great-grandmother was dead. Slowly Megan releases the fantasy and acknowledges that she is alive. As the sessions progress she emerges from the encasement of her great-grandmother’s clothing like a butterfly. She draws a butterfly in her Self Image; she feels herself coming to be released from the cocoon, fragile but beautiful and free, with many possibilities. In contrast, she says of her first Self Image, drawn two months earlier, “Black and red center, an image of hell.” Her attitude and general demeanor are softer as the anger is dispelled. While she feels sadness about her family, it is an honest confrontation with some of the real issues. She realizes that her mother was working to support the family, a role she assumed because of financial pressures. The profession Megan would be entering is dominated by men and she
Clinical Applications — 67
was afraid of further losing her feminine identity in such a setting. She admitted that her mother, while wearing suits in the same profession, is not a male-looking figure. Megan feels she can hold her sexual identity constant. Megan says, “I have a number of ‘image’ problems to work out, but I’ve identified a lot of the problems and gotten in touch with what the ‘tools’ are.” In follow-up sessions she reported to the therapist that she was being seen in therapy weekly and appeared to have stabilized her gains.
Summary
1. The verbal test measurements improved with the passage of time. The variables of her Physical Body and Self Satisfaction increased and showed more flexibility, more realism, and more positive feelings both toward herself and others. She was better able to care for and about herself, emotionally and physically. 2. The Verbal Assessment in response to her Eating Questionnaire was more positive and realistic. She was able to stabilize her image in the mirror and recognize herself. Her identity as a female being emerged. 3. In her art work we see a more delicate use of color, better composition, more harmony, and integration, resulting in a more significant form. The drawings express softer, less pressured feelings and identification and acceptance of her femininity as well as her masculinity. 4. There appears to be a correspondence between the results of the Phenomenal and Nonphenomenal Tasks. The changes noted in the TSCS, Eating Questionnaire, and her weekly Self Reports indicate a more realistic attitude, recognition of her self-concept, and emerging positive selfesteem. The second series of female figure drawings, the Mandalas, and the Body Contour Drawing are more aesthetic, more expressive, and psychologically healthier. Megan is reaching toward her maturity, more acceptance of her strengths and her wholeness. She notes her own progress: The mirror is not the enemy it was six weeks ago. I am not ashamed or embarrassed to look into it. . . . I still hate my ass, hips, and thighs, [but] eating is not my first choice anymore. . . . As I lower myself into the hot, pretty, scented bath water, I think “I am my body.”
68
— Clinical Applications
Jessica Mason Tennessee Self Concept Scale (TSCS) Data Analysis
Jessica Mason’s Self Criticism Score (SC) is 42 on both pretest and posttest, registering at the 80th percentile. Her SC score indicates a normal capacity for self-criticism and is consistent with the results of her Total Positive Score (P), giving credence to and supporting the positive scores. Jessica’s P score on pretest is 331, a reading at the 28th percentile. Her posttest, administered two and a half months later, rises to the 93d percentile with a P score of 387 points, an increase of 56 points, and a rise of 65 percentile units. Jessica’s pretest score for Physical Self is 53; posttest, her score rises to 72, a gain of 19 points, bringing her score from the 0.8th percentile to the 45th, an increase of 44.2 units. Jessica’s Self Satisfaction Score pretest is 101; posttest, it rises to 126, a gain of 25 points. This represents a rise from the 39th percentile to the 95th percentile in Self Satisfaction, a gain of 56 percentile units. Her score for Personal Self pretest is 51, a reading at the 4th percentile. Her posttest score for Personal Self is 75, a gain of 24 points, raising her score to the 91st percentile, a gain of 87 percentile units. Jessica’s Variability Score (V) pretest is 64; on the posttest her reading is 50, a drop of 14 points, in general a more favorable result, indicating less inconsistency between scores from item to item. The Distribution Score (D) was 151 in the pretest and 139 in the posttest, a reduction of 12 points, indicating a more secure feeling about the way she sees herself. (See appendix 1a for an overview of scores for Personal Self, Self Satisfaction, and Physical Self.) Jessica’s Time Score was thirteen minutes in the pretest performance and nine minutes posttest, well within the normal limits. In summary, Jessica improved her total P score from the 28th to the 93d percentile and made significant gains in the individual variables. (See figure 5.7 for a comparison of Jessica’s first and second TSCS results.) Jessica was referred to this study by her physician. At the screening interview Jessica stated that she wished to be part of this study because “I’m happy about my life. I’m not happy about how I look . . . never felt bad enough to seek help . . . like to like myself . . . I’d
Raw Scores
—
121
138
101 126
109 123
53 72
81 87
51 75
72 87
66
74
50
64
31 22
28
33
151 139
Pretest Posttest
T —95 — — — — —90 — — — — —85 — — — — —80 — — — — —75 — — — — —70 — — — — —65 — — — — —60 — — — — —55 — — — — —50 — — — — —45 — — — — —40 — — — — —35 — — — — —30 — — — — —25 — — — — —20 — — — — —15 — — — — —10 — — — — —5
by permission of the publisher, Western Psychological Services, 12031 Wilshire Boulevard, Los Angeles, CA 90025.
Answer-Profile Sheet (W-182B) copyright © 1964 by William H. Fitts. Reprinted from the Tennessee Self Concept Scale
Jessica Mason: Comparison of Results of First and Second Tennessee Self Concept Scale
331
387
42
0.01
JESSICA MASON
0.01
42
0.1
1
0.1
5
5
1
10
10
Tennessee Self Concept Scale Pretest (13 Min.) Posttest (9 Min.)
20
20
Percentile
70 60 50 40 30
D
80
Row Total V
70 60 50 40 30
Column Total V
80
Total V
VARIABILITY
95 90
Column E Social Self
95 90
Column B Column C Column A MoralPersonal Column D Physical Self Ethical Self Self Family Self
99
Row 3 Behavior
POSITIVE SCORES
99
Row 2 Self Satisfaction
99.9
Row 1 Identity
99.99
Total Positive
99.9
Self Criticism
99.99
Percentile
Figure 5.7
95— — — — — 90— — — — — 85— — — — — 80— — — — — 75— — — — — 70— — — — — 65— — — — — 60— — — — — 55— — — — — 50— — — — — 45— — — — — 40— — — — — 35— — — — — 30— — — — — 25— — — — — 20— — — — — 15— — — — — 10— — — — — 5—
T
70
— Clinical Applications
like to care about myself as much as the people I love.” Jessica is a thirtysix-year-old white woman, weight 183 pounds, height 5 feet 3 inches, and has a small body frame. According to the Metropolitan Life Insurance weight tables, this is about 60 pounds over the recommended weight for her height and body frame. She is intelligent, articulate, and pretty; her most striking feature is her eyes, which are bright and expressive. She has a broken front tooth. . Jessica is a housewife and has two young children, two and four years of age. She has been married for six years to Ralph, who is employed in his family’s business. Jessica was born in New York, where she has lived all her life. She had six months of college, having art as a background. She was employed as a film editor before her marriage and has since then occasionally worked freelance in this field. . Jessica’s weight became a problem at nineteen years of age. In the past, in addition to working with the referring doctor, she participated in the Weight Watchers Program. She lost eighteen pounds following that regimen and then regained twenty-two. She subsequently followed the Stillman Diet, losing twenty-seven pounds, which she kept off for three years. After her marriage she regained all the weight. Jessica reports her husband is very overweight. Both children are very slim. . Jessica reports having been a premature baby, weighing three pounds at birth. At thirteen she broke her leg, which was in a cast for six months. She had surgery to correct strabismus at five and again at seventeen; the condition is now stabilized. At eighteen years of age she smoked marijuana as a “recreational drug.” At thirty-five she had surgery to remove her gall bladder. Jessica’s condition was diagnosed by the referring doctor as “obesity due to excessive caloric intake.” The treatment prescribed was diet instruction, but she discontinued treatment. Her doctor reported that no significant result was obtained, as the patient was “poorly motivated to lose.” No other significant medical problems were reported. . Her mother, who is sixty years old, had a heart attack at age fifty-three and has Mackowitz Syndrome (which is similar to Lupus). Jessica’s mother is overweight. Her father, sixty-seven, has hernia and prostate conditions but no other significant health problems.
Clinical Applications — 71
Jessica’s sister, four years her junior, is a nurse and is married. As an adolescent the sister had a serious illicit drug addiction that was the source of many problems for the family. During this period Jessica suppressed her own considerable talent so as not to appear better or more capable than her sister. This profoundly affected Jessica’s self-concept, creating confusion and self-doubt. The sister is no longer abusing drugs. Project Compliance
Jessica was assiduous about keeping appointments and working on the prescribed tasks during the sessions, with very little resistance to completing each task. She used the insights gained through the experiences in therapy to her advantage at home with her family and friends. Initially, Jessica had reservations about her ability to sustain contact over the length of the project. She developed a good relationship with the therapist, began to look forward to the sessions, and became actively involved in the work. At times it was very difficult for her to make arrangements for the care of her children, but she kept all appointments except one, which she rescheduled. In a period of four months she had fifty-five hours of treatment. Though each session was long—about two and a half hours—she was able to sustain attention and energy throughout. In the sessions she addressed herself to the issue at hand with vigor, interest, and intelligence. She worked at home as well on the mirror task and written reports. Her general health was good throughout the project—she reported only one severe headache. Phenomenal Tasks
. Initially fearful, Jessica gradually became less so during the weekly weighing and began to accept it as the reality of what she weighed. At one point she remarked, “It’s what I weigh. I can weigh less if I want to. I can even weigh more if I want to, but it’s what I choose, and it doesn’t matter because I know what I look like. I really know.” She joined a weight-loss program three weeks after the start of the project and lost several pounds, but said she felt it was premature, that she needed time to get to know her body. Although she did not continue to lose weight, she continued to attend the weight-loss group. She stabilized her weight and maintained it at that level until the end of the project.
72
— Clinical Applications
Although her weight did not vary more than four pounds during the course of her involvement with the project, she reported that several people remarked on how well she was looking—that her “weight loss” was becoming. When she asked them how much they thought she had lost, several people on different occasions guessed fifteen to twenty pounds. Jessica also reported several instances when men working on the street in construction jobs whistled and flirted with her. These events were explored with Jessica and her feelings concerning issues that related to her sexuality were discussed. Outraged at first, she then acknowledged that she was pleased by this turn of events. As we view her pictures we can see her emerging sense of femininity and sexuality. This was also evidenced in the change in her appearance as the sessions progressed. A similar theme is noted in the change from the first series HTPPA pencil female figure, which depicts a young adolescent, to the second rendering, which shows a mature, attractive woman close to her own age (see figure 5.8). , . Jessica was able to accept her face and especially her eyes, describing them at various times in her weekly Self Reports as “beautiful, pretty, fine, lovely—I love my eyes.” At times her hair and makeup were rather haphazardly styled, and occasionally she appeared poorly groomed. In the early sessions her eyes were meticulously made up with a complex layering of eyeshadow in many colors. Though skillfully blended for the most current effect, it gave her eyes a somewhat startling appearance. Jessica’s eyes were of special significance to her. Until she was seventeen, she suffered from crossed eyes (strabismus) a condition that resulted in much ridicule by her peers both in elementary and high school. She stated that her feelings of low self-esteem emanate from this period. As she progressed in therapy, her physical appearance altered. She had several haircuts during the course of the project, changing each time to a more sophisticated look. The clothing she wore to the later sessions was more attractive and feminine, switching from pants to dresses. Her earrings matched, and her eye makeup softened, resulting in a more integrated and harmonious appearance.
Clinical Applications — 73
Figure 5.8
—
Jessica Mason: Pencil Female Figures from HTPPA Comparison of first (left) and second (right)
During the course of the project she spoke of the fact that she had been asked to be PTA president at her child’s school and discussed her fears about directing the necessary programs. She accepted the job before the end of the sessions and handled a large school event successfully, receiving much positive feedback from the school administration and the parents. , -. At the outset of the study Jessica was unable to sustain looking at herself in the full-length mirror for even a few seconds. At those times she would be very negative and critical about her mirror image. In contrast to the positive feelings generated about her face in the hand mirror, in viewing herself full-length at home she wrote: I’m big and grotesque. I don’t look normal. The girl I see is very unhappy. She feels ugly and helpless. I hate my body naked. I hate my hair! Hate my lumps. My body looks strange. . . . None of the parts looks right together.
74
— Clinical Applications
Very ugly all over. . . . Even my face changes, some days it looks nice and some days . . . other days it looks like part of my body—fat! My body looks like an old person’s, all hanging down and loose and horrible. . . . I feel like it’s hopeless . . . it’s too much.
It was as if she were two people viewing herself, one from the neck up and the other from the neck down. She usually appeared in casual clothes, sandals and baggy jogging outfits (although she did not jog). Out of keeping with this informal look, there was much jewelry, rings on many of her fingers, and always lots of bracelets. She consistently wore earrings that did not match, giving her an aesthetically unbalanced look. As time went on, she was gradually able to view herself in the fulllength mirror in a less judgmental way. Three and one half months into the project she said, “Now I know what I look like. I really know, and I don’t look as bad as I thought. As a matter of fact, there are days where I think I look damn good.” ₍₎. In doing the measurement tasks, it was evident that Jessica was unable to judge size accurately. In the tissue box task (see chapter 4 for a description of the task), her estimate was off from one to two inches in all dimensions. This problem was confirmed in the task that required her to guess her own body dimensions. She estimated her total linear measurement to be 160 inches; her actual linear body measurements totaled 120 inches. Jessica had overestimated her linear measurements by a total of 40 inches. It is interesting to note that while she distorted the measurements in guessing her overall body length, she most grossly distorted her guess for upper leg from hip to knee by nine inches. And, while she underestimated her roundness overall, she nevertheless overestimated her upper leg roundness measurement by eight inches, this, the same area of overestimation in the linear measurements. During a mirror-viewing session early in the project, in discussing various feelings about her body, she had said, “I think my legs are the part I hate the most—lumpy, veiny, white, splotchy, fat, and ugly.” The BDEM Task was the most difficult for Jessica to deal with, as she did not wish to know her size. Facing this with the therapist present in an atmosphere of support, and with a nonjudgmental attitude about the
Clinical Applications — 75
reality of her weight and size, helped her to overcome her revulsion about her body. The repetition of some of these tasks helped to rid her of her phobic attitude about her looks and her shape. At the end of the twenty-two sessions Jessica was enabled to recognize her inability to accurately assess amounts and sizes. She tells the therapist that she had always served 16 ounces of steak as a single portion to herself and a similar portion to her husband for dinner along with the rest of the meal. She had always assumed that this was a normal “portion.” She began to weigh and measure amounts and will need to do so until she learns how to sense and feel. In addition to a lack of ability to judge portions by sight, she was unable to identify her own hunger or satiety. Eight weeks into the study, Jessica related that she was starting to recognize hunger and was better able to manage her eating, both at home and eating out at friends’ or at restaurants, by trusting her ability to know what her body was saying and asking herself the question “What do you want?” Nonphenomenal Tasks
₍₎. Jessica’s self line in the first rendering of the CFLD is a heavy red the same size as her husband’s. She titles it “My Family.” She says she was going to call it “The People I Love” but, “because I’m in it, I can’t call it that.” She explains that the use of red for her self line is “because I’m mercurial, I change my mind a lot.” In her second CFLD her line is green and slender and more appropriate in size in relation to her husband’s. The green line may represent a sense of her growth and renewal. Twelve weeks into the project she announces, “I feel my life just started. I feel wonderful, I can’t wait to wake up in the morning. I feel like I’ve gone through a rebirth.” ⁄ ⁄ ⁄ ⁄ ₍₎. In assessing Jessica’s HTPPA from the first to the second series, there is a general trend toward more natural drawings, less rigid in stance, and more mature figures. Her first chromatic house is childishly executed, facing front; a chimney appears, but no smoke; there are clouds overhead. The second chromatic series shows a more complex house with many levels, indicating some of the levels of her Self that have been revealed through the project. A large glass sunroof allows light into her room, and there are safety escape devices in the stairways leading from the top (see figure 5.9).
76
— Clinical Applications
Figure 5.9
—
Jessica Mason: Chromatic House from HTPPA Comparison of first (top) and second (bottom)
Clinical Applications — 77
The first pencil tree is an apple tree with four apples, one for each member of the family. It is cartoonlike and static. The second pencil tree drawing she calls a “willow” tree. It appears sensuous and graceful with many facets. She says of this tree, “It is flexible, it moves.” (See figure 5.10 for a comparison of Jessica’s first and second pencil tree drawings.) Her first pencil female figure, drawn in outline, is childish and has doll-like hands and feet in what appear to be slippers. The second pencil female figure is a more realistic drawing. It is a mature young woman very close in age to Jessica’s real age; the line is fluid, the body full and sensuous, the eyes directed inward. It is a little off balance, perhaps in response to the exploration of the Self revealed through the tasks. (See Figure 5.6 for a comparison of Jessica’s first and second pencil female figures.) In her first chromatic female figure a ten-year-old child jumping rope is depicted; seven weeks later Jessica drew a slim, stylishly dressed, mature woman in an attitude of assurance. Animal drawings, like human drawings, represent the person’s feelings about himself (Hammer 1958). Feelings of largeness, clumsiness,
Figure 5.10
—
Jessica Mason: Pencil Tree from HTPPA Comparison of first (left) and second (right)
78
— Clinical Applications
awkwardness, uncoordination are often related to the individual’s selfconcept. Physical attachments seen in long-necked animals like the giraffe, elephant, whale, anteater, sucking insects, and the seahorse depict feelings of strong oral attachment, like the umbilicus. These are condensed symbolic forms that may be seen in individuals with dependency problems. Jessica’s four animal drawings may be an index to her conflict about being a grownup able to assume adult responsibilities. Her first animal pencil drawing is of a dog Jessica describes as “peeing in the children’s room—mischievious—he moved in with my husband.” She identifies this dog with her real dog, and labels the drawing, “My First Child.” The dog suffers from epilepsy, a condition that affords him special care, and is forgiven his transgressions because he is disabled and not responsible for his actions. This drawing may be a depiction on some level of the feeling Jessica has about herself, suggesting her feeling that she has a disability (her obesity), something over which she has no control that causes her to do inappropriate things. The drawing showing the dog (herself) in the act of urinating in the children’s room is perhaps also depicting her conflict about the care she gives to her children and her own dependency needs. She expresses these feelings numerous times early in treatment. “I don’t like being a grownup. It’s very hard to be grown up and I felt like a helpless child.” And again, “I didn’t understand how hard it was to be a parent.” Her first chromatic animal drawing, now showing a deeper level of her feelings, depicts a giraffe—a long-necked animal—drawn as a passive toy, emphasizing the dependency image. Jessica describes the giraffe as a female who is in a zoo and “thinking about running across the open plain—doesn’t want to be in the zoo.” Jessica’s second series HTPPA animal drawings show growth and a good prognosis. In her second series the pencil animal is a beautiful swan floating on the water. It looks very strong. The swan, with its long phallic neck, is masculine, yet in its rounded, silky body it is feminine, a union of opposites (Cirlot 1971:322). For Jessica it is her acknowledgment of both her inner strength and her sexuality. Jessica says of this: “The swan is feeling the sun on her feathers and going to the supermarket buying grain for the babies.” Although the swan, like the giraffe, is also an animal with a long neck, perhaps indicating dependence, it has been trans-
Clinical Applications — 79
formed into the caring and giving role, a beneficent animal. Also, the swan has evolved (much like the ugly duckling) from a male dog in the first drawing who is naughty and irresponsible and disabled, to a caring, beautiful, and feminine creature who is admired and has fairytale qualities. She says: “I feel like I’ve gone through a rebirth. . . . I feel solid.” (See figure 5.11 for a comparison of Jessica’s first and second pencil animal drawings.) For her second chromatic animal drawing Jessica draws a perky and alert cat, a more typical choice for a female. Of this animal Jessica says: “She’s easygoing but careful. She’s open but not stupid or vulnerable— there’s part of me in this cat.” The cat with a long tail is poised and ready, looking well grounded but active and alive, suggesting a good prognosis in this series. . Jessica’s first Self Image is of a group of images that include a heart, a mouth, and a spiral, all floating in the circle without order or integration. Her second Self Image uses the same elements but organizes them into a coherent whole. The second drawing shows the face of a woman with eyes like Jessica’s and long, flowing hair. The many colors create a soft rainbow effect and give the whole an appearance of beauty. It is a foreshortened view. She titles it “Rising,” and says, “My body is following my head. I’m coming up.” The first Body Image Mandala shows two views. The first is of a little girl, drawn as a bare outline without expression, like a cartoon character, similar to her first responses to the tasks. Jessica insisted upon doing a second drawing in an effort to show her “true” self. This Body Image depicts a naked woman, fat and empty, as if she has been laid bare, perhaps a reflection of the therapeutic encounter of being herself—laying herself open to reality and truth and therefore vulnerable. Of the second Body Image she says, “I don’t have to make myself grotesque to show myself.” She calls it “Rooted,” and says: I feel solid, strong, centered. My head is part of my body. I thought I was normal, but there were two parts of me acting independently. I found out I was a better person than I thought I was. I thought I wanted to be thin, but that’s not all I want. I’m concerned about my brain. I want to be a little more every day. I feel my life just started. It seemed to happen in a subtle way and I feel it’s always been there and it seems normal. I don’t feel awkward in my body.
80
— Clinical Applications
Figure 5.11
—
Jessica Mason: Pencil Animal from HTPPA Comparison of first (top) and second (bottom)
Clinical Applications — 81
₍₎. For her first SB Jessica chose a round oatmeal box with a picture of a Quaker man on the outside. In creating her collage, she left the outside of the box in its original state, except for one picture of a woman’s face which she pasted over the picture of the Quaker, partially covering the image, creating a single face from the two pictures. Her struggle with identity is manifest here. Inside the first SB she placed many pictures that she had clipped from the magazines presented by the therapist, loosely piling them into the box without order or pasting. The second SB is more integrated. She says: “The flowers on the inside are to show the flowers on the outside are a continuation. Before, I’d show a facade, use makeup. What’s going on on the outside is coming from the inside. It used to be the opposite.” In this connection she discusses the movie Tootsie with Dustin Hoffman portraying a woman: In becoming a woman, he found that women are discriminated against and felt as much like a woman in what he went through as any man would. Somehow this symbolizes how I’ve gone through something comparable. I’ve transcended a barrier. I went from hating myself to loving myself. That’s as amazing to me as a man being a woman. In this statement she is talking about her discovery of her own sexuality.
(See figure 5.12 for a comparison of Jessica’s first and second Self Box.) . Jessica’s first Sandworlds had both a fence and a stone wall— there were many items, including a clown. The grouping was unbalanced, giving a lopsided appearance, much like her own feelings of being offcenter, which was also reflected in her dress. The second Sandworlds was a balanced group in mandala form. Of this she says: “I wanted it to be a circle with things I was afraid of not understanding—I’m not afraid.” The clown, which appears in the first Sandworlds, is knocked down here, indicating that it is no longer a threat. She says: “I’m an overweight woman, not a fat lady in the circus.” ₍₎. In this task Jessica depicts a scene from her childhood, “The Day We Bought Gigi.” She describes this as a happy memory concerning the dog her mother and father bought for her when she was ten years old. During this exercise Jessica makes the connection that she had always deferred to her sister and family so that she
82
— Clinical Applications
Figure 5.12
—
Jessica Mason: Self Box Comparison of first (left) and second (right)
would not appear to be better than her sister. Her sister’s involvement with drugs made Jessica feel guilty—that somehow Jessica did not deserve to do well and look well. She says, “I made myself less perfect” so as not to perform or look better than her sister. In the sculpture Jessica is seated on the floor, at the level of the dog, a puppy. The other members of the family, including her sister, are standing. As in her pencil animal drawing, she identifies with an incontinent dog. The KFCS releases feelings and illuminates the meaning of certain events. She faces her grief over the death of her husband’s grandmother, which had occurred the previous year. “Granny” was the significant person in Jessica’s daily life and had become her surrogate mother. In the second KFCS, when asked to “make it better,” she leaves out the family and stands alone in the sculpture with the dog Gigi. In pro-
Clinical Applications — 83
ducing this image she realizes that she was a significant person who could have an impact without the family and deserved to stand on her own—a recognition of her inner strength and emerging maturity. In reviewing her art productions at this point in the project, she observes, “I learned here about caring about myself and my distortion of myself.” Combined Phenomenal and Nonphenomenal Task
₍₎. The first BCD is much like the first picture in the HTPPA series, which is static and sterile, lacking expression and feeling. In speaking of this picture, Jessica says, “It’s like a cartoon.” The drawing is done in magic markers and, while competent, lacks the aesthetic art quality that her drawings in the second series show. In the second BCD we see Jessica’s transformation and breakthrough clearly. The drawing is done in paints and pastels, both more fluid and risky mediums than the markers used in the first BCD. The picture is a beautiful rendering of a young and vibrant woman, alive. Jessica says, “She could take a step.” (See figure 5.13 for a photograph comparing Jessica’s first and second Body Contour Drawings.) After these drawings she asks the therapist, “How come I’m not anorectic? I saw myself as fatter than I was.” She compares her first BCD with the second made one month later: [Of her first Body Contour Drawing]: It was like drawing a paper doll. . . . I knew that it was me, but it was flat—I was drawing a picture inside a picture. . . . I knew it was me, but I didn’t accept it. It was like a cartoon. . . . I tried to make everything exactly right, I was very literal—but it didn’t look anything like me. I worked so hard to stay in those boundaries and I was all over the place. . . . I didn’t know where the lines were. [Of her second Body Contour Drawing]: The person that I was working on had a circumference . . . those arms were really arms, and when I was painting the inside of the jumpsuit it was like my body was in there. I accepted that as me. The second one was me—I was just drawing what I felt like or who I felt I was . . . I didn’t think about what it looked like, and it looked like me. . . . It’s amazing to me because now I’m so real to myself and so true to myself that even when I let go, I’m true. . . . That gave me the liberty to abstract it, because I knew what it really looked like so I was
84
— Clinical Applications
Figure 5.13
—
Jessica Mason: Body Contour Drawing Comparison of first (left) and second (right)
able to make my hair a little longer than it was or draw my face a little differently. . . . Everything is the same, except it seems easy. I just feel calmer. . . . I’m less upset by little things.
Self Report
. Three weeks before the completion of her participation in the project, Jessica recorded on tape some of her feelings related to the study. (See appendix 1a, Extracts of Exit Tape Recordings.)
Clinical Applications — 85
. See table 5.2 for a comparison of Jessica’s responses to a series of questions on her first and second Eating Questionnaire. Discussion
During the course of the project Jessica comes out of the “illusory orbit of oneness” (Kaplan 1978:273). Jessica states, “I feel I have gone through a rebirth.” Her second birth is at hand, the psychological birth,
Table 5.2
—
Jessica Mason: Comparison of Responses to Eating Questionnaire
Question
Answer 1
Answer 2
What is your eating problem?
I eat whenever I want to whether I feel hungry or not—I don’t even think about whether I’m hungry— if I’m offered something I like, I’ll eat it until it’s gone and feel very bad about it while I’m doing it, but I don’t stop.
I don’t have an eating problem, but I overeat at times.
What do you believe to be the cause of your eating problem?
My laziness to get control, to stop, to have the strength to say “no” to myself.
A lack of love for myself.
How does your eating problem affect your life functioning?
It affects my attitude toward myself and the things I do, revolve around my unhappiness with myself and how I look.
Does not.
How do your life problems affect your eating?
I eat whether I’m happy, sad, it doesn’t seem to be worse or better in regard to my stress.
I deal with my problems by talking or action— they don’t affect my eating anymore.
At this time, are you:
Gaining and losing: I’m up and down—I’m not motivated to get going once and for all.
Weight stabilized. I’m just getting used to the way I look—I need time.
Sad.
Good.
1. gaining weight? 2. losing weight? 3. weight stabilized? How does this condition make you feel?
86
— Clinical Applications
which she may not have appropriately achieved during the course of her early development and now experiences through the tasks. Becoming aware of her body boundaries through the many ways explored, she defines her body both physically and psychologically. She establishes her orbit in her environment—her needed physical and psychological space. In so doing she comes into possession of her rightful place in the world, both its breadth and width, and, in the process, discovers its limitations as well. This is her maturation. Her initial assertion at the outset of the project that she was vaguely “happy” is like the undifferentiated “infant smile” (Kaplan 1978:10). Through the art work, over time, she becomes more specific and is able to identify both her body and feeling states, positive and negative, with accuracy and direction. She becomes better able to maintain or improve them. That fragile line between the fear of aloneness and the need to be separate is managed when the concept of object constancy is belatedly achieved. She learns that the love of the significant people in her life can be constant even when their presence is virtual. Her body image and self image become congruent as she progresses from the stage of actualization of the body, by its sign, to visualization through the illusion in the mirror, to symbolic transformation. Expressive virtualization through the art work brings her to the final stage of authentic symbolization, which incorporates the memory of the physical being. She begins the work of reconciliation with her outer being. Summary
1. The verbal test measurements changed positively from the beginning of the project to the end. Her physical body as depicted in the pictures showed growth and maturation, more flexibility, sexuality, realism, and more positive feelings. 2. Self Reports in the Eating Questionnaire changed. She was able to recognize her physical self in the mirror and allowed her psychological self to emerge. Her inner Self, which she initially called a “mouse,” now is large and capable—not fearful. She now views herself as “a woman, no longer a fat lady in a circus.”
Clinical Applications — 87
3. In assessing her art work we see aesthetic as well as psychological changes: toward more significant form and more positive expression, better use of color and composition. 4. There seems to be a correlation between the verbal aspects: her improvement in the TSCS scores, the change in the Eating Questionnaire responses, and the Self Reports, which show positive feelings, and the nonverbal: the Self figure drawings, Mandalas, and the Body Contour Drawings, which are more aesthetic, expressive, and positive. There is more integration, organization, clarity, and maturity. Her progress is evident in her willingness to take risks and to test her freedom within form. She says, “Even when I’m free, I’m true, and I don’t go out of bounds.”
Claudia Bernard Tennessee Self Concept Scale (TSCS) Data Analysis
Claudia’s Total Positive score (P) pretest is 344, posttest, performed eleven weeks later, it rises to 363, an increase of 19 points. This represents a change from the 42d percentile to the 68th percentile, an increase of 26 percentile units. Claudia’s Self Criticism score (SC) is 42 on the pretest and drops to 34 on the posttest, a reading in the 48th percentile. Both scores are within the normal range for this item. The variables of Self Satisfaction, Behavior, Physical Self, and Social Self show improvement. On pretest in Self Satisfaction Claudia scores 106, in the posttest it rises to 115, an increase from the 59th percentile to the 75th. In her Behavior score, pretest is 112, posttest it is 120, a rise in this variable from the 40th percentile to the 68th, a gain of 28 percentile units. In the area of Physical Self, Claudia’s initial score in the pretest is 65 and in the posttest it is 73, indicating a change from the 21st percentile to the 52d, a rise of 31 percentile units in this important area. Claudia’s score for Social Self is 68 pretest, and 74 on the posttest, rising from the 47th percentile to the 77th, a gain of 30 percentile units. Her Variability (V) score, which is 70 in the pretest, drops to 58 in the posttest, a loss of 12 points, a more favorable score, indicating a less
88
— Clinical Applications
compartmentalized self-view overall. Her Distribution score (D) pretest is 131, and posttest 125, both within normal limits. Her Time score pretest is twenty-three minutes, three minutes over the normal limit. It drops to twenty minutes in the posttest, bringing the score into a better time frame. In summary, at the termination of the project Claudia increased her total P score from 344 to 363, representing an overall increase of 26 percentile units, and made significant gains in the areas of special interest to the study, i.e., Behavior, Self Satisfaction, Physical Self, and Social Self. In addition, her view of herself from variable to variable was modified and made more consistent from item to item (see figure 5.14 for Claudia’s TSCS pretest and posttest results). In assessing the results of Claudia’s TSCS, it should be noted that she is forty-six years of age, in the upper range (60) for which this scale has been validated. Thompson (1972) says that older people usually have a more secure self-concept, though it may be due to denial. They would therefore tend to have a higher initial score and gain less compared with younger subjects. Claudia’s results bear out this hypothesis. Claudia was referred to the project by a friend who was herself a research subject in this study. She describes her reason for participating at the screening interview: Due to stress, I’ve been very self-abusive as far as my eating habits are concerned and my other habits—[need] to be self-supporting financially— I have not been able to help myself overcome my stress. I’ve made attempts to look for work, to lose weight. I can’t seem to take a step to change things. I would like to be in charge of my own life and to regain my motivation and enthusiasm for life and survival. I have things bothering me. I’m confused, that’s the problem. I feel I’m all alone in this world—a lot of deaths in the family. I had to be strong, my family did not come—if I died they would come.
Claudia told the therapist that she was thirty-five years old, admitting later to having lied about her age, which was actually forty-six. Though she admitted she often does this, she decided that in this instance she “would be honest” because “it was important, the same as going to a doctor.” Claudia is a white single woman, 5-feet-6-inches tall. At entrance to the study she weighed 161 pounds. According to the Metropolitan Life
Raw Scores
126
128
106 115
112 120
65 73
78 81
59 61
74 74
74
68
70 58
30
40
28
30
131 125
Pretest Posttest
T —95 — — — — —90 — — — — —85 — — — — —80 — — — — —75 — — — — —70 — — — — —65 — — — — —60 — — — — —55 — — — — —50 — — — — —45 — — — — —40 — — — — —35 — — — — —30 — — — — —25 — — — — —20 — — — — —15 — — — — —10 — — — — —5
by permission of the publisher, Western Psychological Services, 12031 Wilshire Boulevard, Los Angeles, CA 90025.
Answer-Profile Sheet (W-182B) copyright © 1964 by William H. Fitts. Reprinted from the Tennessee Self Concept Scale
Claudia Bernard: Comparison of Results of First and Second Tennessee Self Concept Scale
363
—
344
42
0.01
CLAUDIA BERNARD
0.01
34
0.1
1
0.1
5
5
1
10
10
Tennessee Self Concept Scale Pretest (23 Min.) Posttest (20 Min.)
20
20
Percentile
70 60 50 40 30
D
80
Row Total V
70 60 50 40 30
Column Total V
80
Total V
VARIABILITY
95 90
Column E Social Self
95 90
Column B Column C Column A MoralPersonal Column D Physical Self Ethical Self Self Family Self
99
Row 3 Behavior
POSITIVE SCORES
99
Row 2 Self Satisfaction
99.9
Row 1 Identity
99.99
Total Positive
99.9
Self Criticism
99.99
Percentile
Figure 5.14
95— — — — — 90— — — — — 85— — — — — 80— — — — — 75— — — — — 70— — — — — 65— — — — — 60— — — — — 55— — — — — 50— — — — — 45— — — — — 40— — — — — 35— — — — — 30— — — — — 25— — — — — 20— — — — — 15— — — — — 10— — — — — 5—
T
90
— Clinical Applications
Insurance weight tables, this is 40 pounds over the recommended weight for her height and small body frame. Claudia is an attractive woman with striking green eyes, dyed red hair, and a bright smile. . Claudia, who has never been married, lives in New York, where she was born. When growing up, she lived in several other parts of the country while her father was in the military. A college graduate, she was a teacher for twelve years but left about seven years ago to pursue a career in merchandising. She has held several other jobs, none for very long. She was fired from the most prestigious of these after about two years. In retrospect she feels she provoked this action because of her difficulty with her boss, a female. Claudia has been virtually unemployed during the last few years. At times she has had to sublet her apartment and live with a friend in order to meet her expenses. At entrance to the study she was working as a babysitter for the minimal hourly wage. She had also borrowed money from her family and was indebted to a friend for providing payment for some of her needs. . As a young child and until twelve years of age she recalls being of “low weight,” eating to “accommodate” her mother. She states, “I was studying ballet, but I was not anorectic.” Claudia reports being visibly overweight by her early teens. At sixteen she was 135 pounds, at twenty she was 130 to 140 pounds, and continued to gain weight, which exacerbated when her father died. Claudia’s physician diagnosed her condition as “exogenous obesity. No evidence of endocrinopathy. I am not optimistic about results without supervision.” Claudia stated that she joined Weight Watchers ten years ago in order to lose weight so she could get a job. She lost thirty-five pounds in six months, but regained all the weight, reaching a peak of 170 pounds. . Claudia was full term, birth weight 5 pounds. She reports chicken pox, mumps, and whooping cough as childhood diseases, an ear infection and allergies. Although she denied suicidal ideation, she stated that she had been in a state of severe depression for three years because of a series of deaths of members of her family and friends. The sudden realization that she had not mourned her father when he died fifteen years
Clinical Applications — 91
before increased her depression. Though depression is noted in her doctor’s report, she has never been in treatment for psychological problems. . Her mother is seventy-two years old, widowed, in good health and of normal weight. Until recently her mother worked as an executive secretary. Claudia reports that she has a close but difficult relationship with her mother, who treats her “like a little girl.” Her father was a gynecologist, always overweight, had ulcers and had “an operation in which part of his stomach was removed.” His sudden death from a heart attack was a traumatic event for Claudia who had been very close to him and considered him her support and adviser. After his death she quit her job as a teacher, which had been the profession the family chose for her. She has been unable to settle either in a job or in relationships with men; she always thought she would be married “some day” and found it surprising that she had reached this point in her life without realizing these goals. Claudia has one sister, seven years younger, who is married and lives in another state with her husband and two young children. Though Claudia reported a good relationship with her sister, there was a growing rift because Claudia had not been able to establish a satisfactory relationship with her brother-in-law, whom she says she really respects. In discussing this, she realized she was expecting her brother-in-law to fill the role of her father. She was awkward, approaching him with a lack of grace and tact, much like the elephant approaching the anthill, an animal she depicts in her first Body Image drawing (see figure 5.15). Project Compliance
Though Claudia was cooperative and determined to complete the project, she found it difficult to comply with the tasks. She was never satisfied that her effort was “correct” and would often repeat the task to “make it better.” Gradually she began to accept her effort as both appropriate and correct. The therapist represented the authority of her mother and her former boss, with whom she was still struggling for control. It took some time before Claudia made these connections. During the course of the project she became more accepting and more realistic of her strengths, her deficiencies, and her accomplishments. In the process she
92
— Clinical Applications
became more accepting of needed focus and structure and was then able to decide when it was appropriate to accept authority and when her own counsel was appropriate. Phenomenal Tasks
. Though the therapist did not encourage participation in a weight-loss program during the course of the study, Claudia decided to join Weight Watchers and lost fourteen pounds. It made a difference in the way she looked and in the way people responded to her. This motivated her to resume some friendships. She also started on a regimen of walking, which made her feel very fit and increased her weight loss. Because her new job was a six-month temporary position, Claudia wanted to stabilize her gains so that when the job terminated she would not lose her good feelings about herself. She was always a little tense during the weekly weighing, as she was determined to lose the weight. , . Claudia stated in an early mirror-viewing session, “I accept the reality of my appearance for the present,” but rejected the image as “not the me I want to be.” Throughout, she focused on her eyes, which she considered as an important and powerful feature that she used as the means to get what she wanted. In her first response to the question “What is your best asset?” she writes, “My eyes. (Sometimes they help me to be ‘charming’ when I want to be or need to be.)” During the early sessions she would often act coy and wheedling, twisting her body and head like a little child, to express what she wanted to say. Later, she amends her answer and says that her best asset is her “personality.” , -. In the early sessions Claudia found it very difficult to sustain looking at herself in the mirror even for short periods of time. She would talk throughout the mirror-viewing and was restless and tense during this exercise, saying that she hated it. As time went on, she became more tolerant of herself. She says, “I feel very proud of myself. . . . I feel very purposeful in all areas of my life and very goaldirected.” She obtained a well-paying job three weeks into the project, and was able to return all borrowed moneys, give up babysitting, and dress in a more sophisticated, and definitely more attractive, manner. Eye
Clinical Applications — 93
makeup was softened and a more integrated makeup application gave her a finished look. She also restyled her hair, eliminating the bangs (which she said she had worn as a teenager). While she worked hard at her new job, she rethought her goals, and registered for several courses directed toward preparation for a professional career in interior design. ₍₎. Though Claudia was able to estimate her body measurements quite accurately, she was unable to hold these assessments constant. She maintained that her image in the mirror was larger than the BCD traced from her body. In reality, the mirror image is one-half the size of the actual figure (see Gombrich 1960:17 for discussion). Her gross denial that she was both what she saw and what she knew served to destabilize her self-concept and left her adrift and confused. This was underlined by her knowledge that she was forty-six years old but unwilling to understand and accept this fact. The distortion in her body dimension/body image was only part of a total fantasy she had created that extended far beyond the single lie of age deception. She seduced herself into thinking that at some level she was, with the complicity of her friends, passing for twenty-eight. She became convinced of this deception and ultimately came to believe it as fact. Now she was not passing for twenty-eight, she was twenty-eight. She was drawn further into the realm of fantasy. Claudia fantasized that she was in her twenties and therefore younger men were appropriate partners, perhaps eligible as husbands. She told the therapist that she began to think that someday her “Prince Charming” would come and she “would be taken care of.” Until that time her life “hasn’t begun yet” (another deception). Psychologically, she believed that her biological clock had stopped in time. The family became entangled in this scenario: Claudia, childlike, was not working and therefore required financial support. She now regressed further; not mourning her father’s death was, in effect, denying his death. She deposited herself emotionally, totally into the outgrown family nest. Feeling its inadequacy, she rebelled, and was in a desperate power struggle with her mother. In the final sessions of the study she began to sort out reality from fantasy. She said, “I don’t want to be in my twenties or thirties” and, triumphantly, “I’m in my life!”
94
— Clinical Applications
Nonphenomenal Tasks
₍₎. Claudia’s self line in the first rendering of the CFLD is drawn in red crayon, as is the entire family. She places herself in the center of the family, next to her mother and sister. The drawing takes up a tiny portion of the page, and all seven members— her self line, mother, sister, aunt, two nieces, and brother-in-law—are contained in an area measuring 1½ by 1¼ inches on a page 14 by 17 inches. In the second CFLD the family groups are separated, as they actually are in real life, living far apart from each other. Claudia’s line is now yellow and purple, and each person is identified by her or his given name. It is a more realistic expression of the family at this time. Of this she says, “It’s different than before—I’m separate.” ⁄ ⁄ ⁄ ⁄ ₍₎. The first series of pencil drawings indicate resistance to the task by the token drawings produced. Claudia here expressed her answer to the therapeutic situation in which the therapist in effect “told her what to do.” Claudia had problems in the past with female authority figures, i.e., her mother and her boss, but in her responses in the first chromatic series we see her capitulation to the process and authentic responses become evident. Here are revealed her dependency fantasies. The first chromatic house is a detailed rendition of her own childhood home. Her longing to return to those times is shown here. Claudia’s depiction of the first series of female figures, much younger than her actual age, is also indicative of her dependency and longing to be cared for. The pencil tree is empty and barren of leaves and has a hole in the trunk, perhaps indicating the trauma of her father’s death. The animal is a mere caricature of a cat, facing front and static. Claudia says, “This cat was neutered, it’s ugly, a very mean cat, unfriendly. I don’t like this cat. I’m allergic to this cat.” In the second series, done two months later, the pencil male and female figures are drawn wearing dark sunglasses. Claudia describes this as “hiding from others while watching them.” She feels she is unseen in this situation, somewhat like the ostrich with its head in the sand. The dark glasses may serve to hide her eyes from the inspection of others; however, they also dull her reception to the brightness of the day. Worn
Clinical Applications — 95
into the evening, they cloud her vision. In the second chromatic series the female figure appears as a mature woman in evening dress, without glasses, and the male figure, also in formal evening dress, is now given clear eyeglasses. Claudia tells the therapist that she has resisted going to the eye doctor to be fitted for glasses. Now, she acknowledges, it is necessary. She calls the second series house “My Home.” It is a drawing of her own apartment, showing the room in which she lives. The tree is in bloom; it has deep roots under the ground. She says, “Maybe the roots need to go deep to hold them in so it will stand up with unseen support. It is late summer, early fall.” The first chromatic tree is described as one hundred years old. She says, “This tree was on my lawn when I lived at home with my parents. It was hit by lightning and had to be cut down. It was a trauma. It represented death. I have an emptiness.” She then discusses her father’s death fifteen years earlier and the fact that she was not allowed a proper mourning time for her father. Her mother would not allow this, as remembering the father upset her mother, and Claudia was resentful. Several recent deaths of family and friends also depressed her. She became very ill with the flu and subsequently gained a lot of weight. She says, “I started flimflamming around. I thought I might be rescued by my prince and did not think of work as a lifetime thing.” Her second pencil animal depicts a turtle. Of this she says, “It is walking toward its goal; the turtle knows it has a purpose, doing what it has to do. Those legs can move pretty quickly. It’s trying to find a mate.” The second chromatic animal is a horse: I should have made a lion. I know how to do that better. It looks like a female with child but not . . . has been inactive . . . has a belly here. It’s exercising, that’s what it’s doing. It’s in middle age. It’s exercising to get in shape, doesn’t want to remain on the farm, doesn’t want to be called a hick, wants to be with it. . . . Reminds me of myself.
Claudia’s first tree drawing, barren and dead, is a memory of death and clearly a connection to the trauma of her father’s death. The tree in her second series is green and reconciles the feeling of dying with both renewal and reality. She says, “The tree is in late summer,” related to the
96
— Clinical Applications
time of her own life as she approaches fifty. She acknowledges her biological clock, saying, “It is certainly late summer, early fall.” Claudia comes to terms with this painful fact. She says she started babysitting “because every time I saw a child I would get tears in my eyes. Every aspect of my life has been giving me sadness. I thought my life had not yet begun because I wasn’t married, but I’m in my life.” Her first HTPPA series shows more fantasy and an unrealistic view of her life, i.e., that her “Prince Charming” would somehow materialize and rescue her. In the second series things are not so pretty, but now they are real. This is the beginning of change, facing up to the reality of her behavior and her inappropriate expectations. She begins to take an active role in her life. Three weeks into the study she applies for a job and is hired in a well-paying prestigious position. She makes contact with several schools as a first step toward acquiring proper credentials to work in the field of her choice. She accepts the fact that, while she is not twenty-five years old and the time for having a biological child is undoubtedly over, she has many years left during which she can be productive and joyful, engaged in a satisfying career and a meaningful relationship. . Claudia’s first Body Image is of an elephant in a jungle. It is sunset. The drawing appears heavy and turgid, the circle contained, floating in a blue sea. In the next session she feels compelled to add a baby elephant to the scene. She calls this “Can’t See the Forest Through the Trees” (see figure 5.15). She likens this to her self-concept, “Feels like a clumsy body, static and stuck, adrift on an island.” One of her key themes is portrayed here: Claudia’s conflict between being dependent and wanting to be considered an adult. The two elephants in the Mandala depict her in the dual role of both being a child and having a child of her own. She now realizes, perhaps for the first time, that she will not have her own biological child, and time has also passed where she wants to go through the process of rearing someone else’s child. She acknowledges her sister’s children, especially the older one who reminds Claudia of herself, as especially precious to her now. She says: I was in a very confused state as to my job direction, my family, my relation with men, being single—the biological clock was approaching an end. I felt ugly, I felt nobody would want me. I felt incapable of doing any
Clinical Applications — 97
Figure 5.15
—
Claudia Bernard: First Body Image Mandala
type of work. . . . My days were unproductive, I was babysitting for neighbors’ children because I had a strong need to be with children and I was getting money for it. It was my only means of support other than money sent to me once in a while by my family. I also did it to escape the reality of presenting my body to others. It didn’t matter with children, I looked a mess every day.
Claudia’s second Body Image, divided into two sections, depicts a young ballet dancer and a horse outside a red structure she labels “Barn.” She calls this Mandala, “Preparing for the Race.” Of this she says: The barn is his home where his food is and where he sleeps. A dancer’s body and a thoroughbred horse are both slick-toned; they really have to eat properly. I’m coming out of the barn—I want to be a more professional person. We have a limited time on earth. A horse has blinders, is more focused. In the past I became distracted. I wanted help. I wanted to live, I never wanted to die, but not interested in making the effort. I’ve started
98
— Clinical Applications
to work towards my goals. This is the interim stage. I don’t feel bad about myself. I don’t feel like an elephant.
Claudia’s first Self Image Mandala is a geometric design divided into four parts. Heavily crayoned and encased in thick lines, compartmentalized shapes appear like the cross-section of a seed pod; it is static and contained (see figure 5.16). Her second Self Image shows butterflies in the four corners of the paper and a peacock in the center in luminescent colors. She says, “A lot of the forms were similar to the first Mandala, but burst open—that was the amazing thing. It showed progress.” Of the peacock, she says, “I wanted to capture the feathers, which are iridescent.” She depicts here an archetypal mandala, luminous in rainbowlike colors. The blending together of all the colors in the peacock is a symbol of totality, the male bird a reflection of her animus, the butterflies in the same picture a symbol of rebirth. She approaches a state of selfhood, the gift of matu-
Figure 5.16
—
Claudia Bernard: First Self Image Mandala
Clinical Applications — 99
Figure 5.17
—
Claudia Bernard: Exit Drawing Center view
rity. She says, “I’m on my way to loveliness. I know I can be lovely, I have been feeling a lot better about myself. I feel different.” In a final picture she expresses this joyous feeling of renewal (see figure 5.17). She draws an exit picture for the therapist that depicts a baby tooting her horn in a large heart-shaped mandala. It portrays her psychological birth, a sign of hope and transcendence. In the corners Fourth of July fireworks appear in celebration of this event. She labels the baby, already partly grown, having hair and an older aspect, ‘’1985” (the year it was drawn) and gives the picture a double title, “Happy New Year” and “A Valentine for You” (although it was summertime when the drawing was made). It is an expression of her feelings for the therapist and for herself, and also her joy at a new chance in life, the beginning of a symbolic new year. ₍₎. Claudia struggled to find appropriate male images to create the first SB. She gives it two titles, “Visions” and “Inner and Outer.” Many images are overlaid, one on top of the other, creating a confused design that lacks cohesion and integration. Eight images in the first SB are of food
100
— Clinical Applications
and eating, in the second only two appear. The second SB is titled “The Emerging Butterfly,” reflecting her sense of rebirth and renewal. It is more contained and focused. Words cut from magazines are pasted on the outside, “Love and Friendship,” and, on the inside, “Awaken the genius in you.” She says of the SB, “It is hard to know the inner and the outer.” ₍₎. In her first SW, called “The Sands of Time,” Claudia selected a number of items that depict childhood: a carousel, a merry-goround, and Santa Claus. Also placed in the scene was a flying saucer and a “robot going into the future.” She says, “I feel like Ferdinand the Bull. I’m excited at cows, I’m the sitting cow.” She is at once a child and also a cow and a bull. Both a child and an adult and both male and female. These symbols succinctly express her conflict. She is an adult who wishes to remain a child and a woman who resists accepting herself as a total person. She is both passive and aggressive, female and male in conflict. In her second SW she says, “The center is the world. I would like to get married, be in a relationship. The person’s coming together. I was a crazy person. I was not in control.” Claudia titles this “Humpty Dumpty Puts Herself Together Again.” ₍₎. This was the most difficult task for Claudia. She did not like to use the clay and found it hard expressing a three-dimensional form. It was a graphic example of her difficulty in facing the many facets of her life and seeing the pattern of her life as a totality from all sides. She abstracted the figures in the first KFCS. In the scene Claudia is the recipient of a prize awarded by the city. Though she was the main character in the sculpture, she says, “I had a passive role. My mother was the dominant figure in the family.” Claudia describes the mother as a “Dr. Jekyll and Mr. Hyde,” adding, “Her bark was worse than her bite.” This task evoked memories of Claudia’s maternal grandmother, the significant positive female in her life. Claudia remembers, “She listened to me. I was very close with her, the matriarch in the family, elegant looking, slim, spoke well, was artistic. I loved her. We were very close. I lived with her until I was three years old.” In viewing the second KFCS, in which Claudia gives the people in the sculpture a representational form, she observes, “I’m no longer a lump.”
Clinical Applications — 101
She learns, too, of her reliance on her father to be her protector. At his death, feeling abandoned and helpless, she became immobilized. Combined Phenomenal and Nonphenomenal Task
₍₎. The two most striking differences between Claudia’s first and second BCDs are the ages depicted, showing a change from a younger person in the first to a more mature person in the second, and the reality grasped, from a cartoonlike rendering in the first to a more realistic and complete figure in the second. After completing the first BCD, Claudia, surprised, says, “I look like a high school student.” She says, “The mirror is more real. In the mirror my body looked bigger.” The reality that her body in actual measurement is larger in the contour drawing than in the mirror continues to elude her at the time of the first drawing, but she anticipates change and says, “This person lives within her body. Things seem to be clearing to my sensibilities.” The second BCD drawing shows an introspective mature woman, closer to her actual age, more expressive and more alive, more feminine and more flexible. The clothing is less constricted, the waist belted, but not too tightly, as in the first BCD. Claudia compares the two BCDs: The contour drawing . . . made me face up to myself. I felt it was a person, and it was me. . . . There were some things I was pleased about and some things I wasn’t, and it pointed up the things that I wasn’t pleased about, pointed up that those were the things that I wanted to improve. . . . It was upsetting. I didn’t like what I saw in myself the first time. I seemed like a child, and I don’t want to be like a child nor did I think I behaved like a child, certainly—I don’t like to admit that I behaved like a child at all, but I realize I do exhibit certain childish behavior: the relationship to my family and perhaps to my own goals. In any case, it’s made me face up to these important changes. The first drawing was a cartoon figure of myself. The second drawing was a drawing of a living, breathing person. There were more details, it was a more human rendition . . . a real person, an analytical person, a person who has certain qualities, good and bad, and who wants to learn about themselves and accomplish what they want to accomplish.
(See figure 15.18 for a comparison of Claudia’s first and second Body Contour Drawings).
102
— Clinical Applications
Figure 5.18
—
Claudia Bernard: Body Contour Drawing Comparison of first (left) and second (right)
Self Report
. Claudia agreed to tape-record her reaction to her participation in the study and to discuss its meaning for her. She prepared for the taping session by writing out some of her thoughts beforehand. Claudia read verbatim from her notes while taping. After completing her prepared script, Claudia asked that the tape recorder be turned on again and she spontaneously added to her original material. (For an extract of her taped remarks, which were made during the twenty-second session, see appendix 1b).
Clinical Applications — 103
. See table 5.3 for a comparison of Claudia’s answers to a series of questions in her first and second Eating Questionnaire.
Discussion Claudia ascends from the depths of despair, which had been rooted in her massive denial of her status related to her age and being single, to a state of hope and promise. She is given a second chance, it is her psychological birth. This is realized in her final spontaneous drawing called “Happy New Year” (see figure 5.17). She feels renewed and hopeful. She says, “I don’t mind being an older woman who looks good.” At fortysix years of age she takes the scary step into adulthood. In so doing, she must renounce the role of dependent child and with it her reliance on others for her nurturance. She now must take over the role of self-feeding and self-care. This may enable her to develop a lasting and meaningful relationship with another. In the past her relationships were transitory. Acknowledging the sad fact of the death of her father gives her permission to mourn him and frees her to establish a meaningful relationship. She also opens herself to the truth that she will not have a biological child and states that she really does “not want it now.” She says, “I don’t have to explain myself to others.” In recognizing her right to be in charge of herself, she is enabled to be more honest both to herself and with others. She says, “I’m beginning to take charge of my life.” She emerges from her cocoon and, though fragile, is at last free. She learns that her family is present as a source within her even when they are half a continent away. She retains their love as a constant and draws strength from that knowledge. The feeling of being willing to be independent is balanced by her need for nurturance. To her surprise, she learns that she is the self-nurturer, capable and competent. It is an exhilarating experience. She feels renewed and wishes to start afresh. She says, “I’m coming back to life.” Claudia brings the therapist a poem that expresses some of these feelings: After a while you learn the subtle difference Between holding a hand and chaining a soul. And you learn that love does not mean leaning
104
— Clinical Applications
Table 5.3
—
Claudia Bernard: Comparison of Responses to Eating Questionnaire
Question
Answer 1
Answer 2
Whom do you admire who is fat?
Winston Churchill, Jackie Gleason. Superintelligent, creative men that have left their mark in history (each in an entirely different way).
No one living. Being fat indicates to me someone with problems (unrelated to food) that they can’t handle.
What’s good about being fat?
It’s childish and immature. I feel guilty saying this, making my mother upset and worrying about me.
Nothing.
What is your best asset?
My eyes. Sometimes they help me to be “charming” when I want to be or need to be.
My personality.
If you could change one thing in your life, how would you?
Being younger.
Go back to school for another degree to prepare me with professional credentials to enter another field.
Describe your eating problem.
I like the activity of eating and cooking and shopping for food. I eat more than I need and eat when I’m not hungry.
It’s not a “problem” now. I’m planning my meals and menus in advance and am being good to myself by not overeating more than I need.
How do your life problems affect your eating?
I eat more. I feel no matter how hard I try, I will fail in all I will do. (Deep down I know that’s not true, but I feel afraid.)
I find I like or want to eat under stress. If I’m happy, to be sociable. But now eat something that will not sabotage my efforts.
Please check your most dominant eating patterns.
Gorging, bingeing, overeating.
Moderation.
Clinical Applications — 105
And company does not mean security. And you learn that kisses are not contracts And presents are not promises. And you begin to accept your defeats With the grace of a woman, not the grief of a child. And you learn to build your roads on today, Because tomorrow’s ground is too uncertain for plans, And futures have a way of falling down in midflight. After a while you learn that even sunshine burns if you get too much, So you plant your own garden and decorate your own soul Instead of waiting for someone to bring you flowers. And you learn that you really can endure . . . That you really are strong And you really do have worth And you learn and learn. With every goodbye, you learn. (Anonymous)
Summary
1. The verbal test measurements showed positive changes, especially in relation to feelings about her physical body. Claudia’s drawings of her body changed from depictions of those of a younger person to art productions that demonstrated increased maturity, realism, flexibility, and openness. 2. Self Reports in response to the Eating Questionnaire changed. As she completes the study she says her eating patterns are self-managed, in “moderation,” and are not a “problem.” Her career goals are directed at establishing credentials that will prepare her to work in a field of her choice. Her inner self, formerly portrayed as an elephant adrift on an island, is now embodied in concepts related to the emerging butterfly, a race horse, and a beautiful and proud peacock. 3. In her art work, changes that reflect subtle but important shifts in her self-concept and body image are evident. There is a more realistic acceptance of herself as a mature adult. There is more integration, better balance, and emerging creativity apparent in the later pictures. 4. The variable of Physical Body in the TSCS and Claudia’s responses to the Eating Questionnaire as well as the taped Self Reports are more congruent and more positive in the posttest. She reconciles her phenomenal or conscious self as a body in space with her nonphenomenal or
106
— Clinical Applications
unconscious body images. The second series Mandalas and the second Body Contour Drawing are reflective of these changes. She accepts both her male and female qualities and lives in harmony with them. She notes her progress by saying, “I’m coming back to life.”
Heather Allen Tennessee Self Concept Scale (TSCS) Data Analysis
Heather’s Self Criticism Score (SC) is 33 on pretest and 34 posttest, virtually no change. Her ability to be self-critical is within the normal range for this item. Her Total Positive (P) is 308 in the pretest, a reading at the 10th percentile. In the posttest it rises to 371, registering at the 72d percentile, a gain of 62 percentile units. Significant gains were made in all the variables. Her Self Satisfaction score, 93 on pretest, increases to 125 in the posttest, a rise of 32 points, representing an increase from the 23d to the 93d percentile, a gain of 70 percentile units. Her score of 49 points for Physical Self increased in the posttest to 62, a rise from the 0.3th percentile to the 12th percentile, a gain of 12 units for this item. Her score for Personal Self, 53 on the pretest, increases to 72 posttest, a gain from the 6th percentile to the 83d percentile, an increase of 77 units. Her Variability (V) Score drops from 76 to 50 from pretest to posttest, a loss of 26 points that indicates a less compartmentalized self-view, a more favorable reading. Her test performance is seven minutes in pretest and nine minutes in posttest, well within normal limits for this item. In summary, Heather’s TSCS score shows a rise in her total P score from 308 points to 371 at the completion of the study and a more moderate result in the item of Variability, bringing her results within more normal parameters. (For a comparison of the results of Heather’s pretest and posttest, see figure 5.19). Heather was referred to the project by the Wilkins Center for Eating Disorders, where she had been a client. She had been given nutritional guidance at the center and had regained some weight. She was experiencing severe anxiety attacks, was unable to accept the weight gain as appropriate, felt overwhelmed by the food, and was in a severely depressed state at the time of referral to the project.
Raw Scores
126
133
93 125
89 113
49 62
76 83
53 72
63 78
76
67
50
76
25
45
31 25
122 132
Pretest Posttest
T —95 — — — — —90 — — — — —85 — — — — —80 — — — — —75 — — — — —70 — — — — —65 — — — — —60 — — — — —55 — — — — —50 — — — — —45 — — — — —40 — — — — —35 — — — — —30 — — — — —25 — — — — —20 — — — — —15 — — — — —10 — — — — —5
by permission of the publisher, Western Psychological Services, 12031 Wilshire Boulevard, Los Angeles, CA 90025.
Answer-Profile Sheet (W-182B) copyright © 1964 by William H. Fitts. Reprinted from the Tennessee Self Concept Scale
Heather Allen: Comparison of Results of First and Second Tennessee Self Concept Scale
371
—
308
33
0.01
HEATHER ALLEN
0.01
34
0.1
1
0.1
5
5
1
10
10
Tennessee Self Concept Scale Pretest (7 Min.) Posttest (9 Min.)
20
20
Percentile
70 60 50 40 30
D
80
Row Total V
70 60 50 40 30
Column Total V
80
Total V
VARIABILITY
95 90
Column E Social Self
95 90
Column B Column C Column A MoralPersonal Column D Physical Self Ethical Self Self Family Self
99
Row 3 Behavior
POSITIVE SCORES
99
Row 2 Self Satisfaction
99.9
Row 1 Identity
99.99
Total Positive
99.9
Self Criticism
99.99
Percentile
Figure 5.19
95— — — — — 90— — — — — 85— — — — — 80— — — — — 75— — — — — 70— — — — — 65— — — — — 60— — — — — 55— — — — — 50— — — — — 45— — — — — 40— — — — — 35— — — — — 30— — — — — 25— — — — — 20— — — — — 15— — — — — 10— — — — — 5—
T
108
— Clinical Applications
At the screening interview Heather describes her fears: Whenever I eat or gain, I hate myself. I feel bad. I don’t feel in control. I feel others won’t like me. I don’t feel pretty anymore. My stomach and my hips make me look like a fat person. Constantly measuring myself every five minutes. If feeling insecure or doubted my existence—looking in the mirror I was in control.
At entrance to the program Heather weighed 122 pounds, height 5 feet 9 inches and of small body frame. According to the Metropolitan Life Insurance weight tables, she was between 15 and 20 pounds under the recommended weight for her height and body frame. Heather is a twenty-five-year-old white woman with dark hair, which she wore in a long, loose fashion. During the early sessions she was continuously throwing her hair back out of her eyes. It was effective as a distraction to conversation. She has large brown eyes, which were exquisitely made up, making them the focal point of her body. Her fashionable clothing was always loose and bulky. Overall, she gave a lovely appearance. She has a soft speaking voice, with a modified Southern accent. . Heather is a college graduate, employed in a lowerechelon executive position in a large company. She is single; at the time of the project she was in the process of ending a long-standing relationship with her boyfriend. She had recently moved to New York from a nearby state. She maintains close contact, through telephoning and occasional visits, with her parents, who still live in a small Southern city in the family home where she was born. Heather describes her worst problem: “Need some relief from driving myself crazy; to have somebody to talk to that wouldn’t get mad or think I was crazy.” . She recalls that as a child she was always skinny but did not feel that eating was a problem until she went to college. She describes the evolution of the anorexia: It was my first semester at college. I had a real hard time, I hated school, and I hated being away from my family. I didn’t get into a sorority, and that just about killed me. . . . About that time . . . I remember looking in the mirror one day and my hipbones didn’t stick out anymore. I just said,
Clinical Applications — 109
“Well, I just won’t have lunch today, I’ll just eat dinner and it’ll go away.” And pretty soon, it was just real easy not to eat breakfast . . . not to eat lunch . . . next, it was real easy for me not to eat until dinner. I could go all day and not even get hungry. . . . I was frustrated at the same time because everybody else around me was going down to breakfast, and they were going down to lunch. . . . I couldn’t understand why I couldn’t eat, too. I would gain weight, but they never seemed to. It didn’t seem fair. I would love to get sick . . . have a flu or virus, because I would throw up . . . that was great. In high school I was never conscious of dieting, but I always remembered feeling conscious of my stomach as sticking out or being big, but it was never translated into skipping a meal. [In college] I could actually control my meals. I didn’t have to go downstairs to the dining room. . . . [I felt] powerful, I could control exactly what my body did—nobody else could do it. I took Exlax every night for three or four years. I wouldn’t let myself eat until I had accomplished everything that day that I had to do. . . . It was a lot of anxiety because my stomach hurt so much. [You can] go so long without eating, then if you put anything into it at all, it’s going to swell or be gaseous and it was a constant cycle of stuffing myself at night and feeling bloated in the morning and then not eating all day to relieve that and then doing the same thing over and over and over. If I had a problem with my mother or I had an upset in my personal life or my professional life, the first thing I would say to myself is “Well, I’m not going to eat, I’m going to lose five pounds.” It was a reaction to everything. I felt so “fat.” I couldn’t go outside, I couldn’t go to the movies. I couldn’t do anything because I felt so awful.
Heather’s physician writes of the treatments he prescribed: nutritional guidance including a maintenance diet, eating program, and balanced diet, aerobic fitness exercise, reassurance, and psychotherapy. His report notes no significant change occurred. She has “behavioral-sexual conflicts between (Southern) upbringing and mores and (Eastern) upbeat lifestyle of her boyfriend.” His impression in relation to her eating disorder: “Seriously neurotic young woman—true anorexia nervosa.” She was in treatment with a psychiatrist, recommended by her physician, but discontinued after four sessions. At that point she was referred to the Wilkins Center for Eating Disorders, which she attended the year before entering the current study.
110
— Clinical Applications
. Heather was born in a hospital near the family home, was seven pounds at birth. As a child she had chicken pox and allergies. In college she had amenorrhea for six months. At times she has overused alcohol and Valium. She was not receiving any medical treatment or psychological treatment at the time of the project. . This is the first marriage for both parents. Her mother, who is sixty-three years old and of normal weight, had Bell’s Palsy, breast cancer, thyroid removed, and a deteriorating spinal disc. Heather has a close but difficult relationship with her mother. Her mother tends to dump her problems on Heather and often creates guilts within Heather for imagined transgressions. Heather’s mother has always placed sexual restrictions on her, possibly because of the mother’s memories of her own premarital abortion. Heather’s father is sixty-three years old and a medical practitioner. He is described as overweight at 200 pounds, has diabetes, and had open heart surgery three times. She describes her relationship with her father as good but distant. She recalls that the first anorectic episode may have coincided with the father’s first heart operation. Heather is one of five children, the youngest of four girls. All siblings are described as slim and all including Heather have scoliosis. Heather reports her relationship with her siblings as amiable, but she was never permitted to develop a close relationship with them. Her mother positioned herself between them to retain the focus on herself. Heather relates episodes of the mother calling her up long distance to complain that her hair was a mess or some other expression of self-denigration. Heather describes her mother as being beautiful, always correct, hard working, and committed to the small-town family stereotype: all is in order. Project Compliance
Heather was aware of the serious nature of her condition. She was so conflicted about her problems that it was a constant struggle for her to comply with her agreement to attend the sessions on a regular basis. At one point, when we considered dropping her application, she telephoned the therapist and asked to reenter the program, describing herself as being in a state of crisis. In despair over the impending breakup with her boyfriend and her inability to cope with her anorexia, she
Clinical Applications — 111
reported an episode, during an anxiety attack, in which she took a large quantity of Valium in a suicidal gesture. Many sessions were spent in long crying episodes of a hysterical nature. This pattern continued throughout the first half of the program. Initially, there was little real interest in the tasks; she was skeptical of their impact. However, her first Body Contour Drawing had a potent effect and marked a turning point for Heather. As she entered the phase in which she repeated the tasks, she had an opportunity to compare her first art productions with the second series. This illuminated some of the underlying process at work and gave her concrete evidence that she was making progress. At times, she missed sessions because of work commitments out of town, but she made an effort to attend sessions, even coming on the weekends. Now she was able to tolerate discussion of some of the dynamics and eventually volunteered her own insights to important issues. Her health during the project was somewhat fragile. She suffered from severe colds and allergies, which seemed to linger. At one point she reported bleeding from her rectum and was advised by the therapist to make an appointment with her doctor, but she did not follow through on this until after the project was completed. In follow-up she reported the doctor found it was a simple irritation that had now cleared up. Phenomenal Tasks
. Heather took the weighing ritual very seriously. Though there was always anxiety about what the scale would show, it was helpful each time for her to see the numbers on the scale. Although she feared that she had gained many pounds from one session to the other, when she saw the actual weight (which did not vary by more than three pounds in seven months), she was initially relieved. Invariably, at the next session, she would exhibit the same anxiety. Facing the weight, she never could make a reasonable connection between what she had eaten during the week and what she weighed. Her ability to make an estimate was always distorted. At one point she insisted that she was eating three meals a day regularly. When asked to enumerate, item by item, what she had actually consumed in a day, it was revealed, much to Heather’s surprise, that though she ate three times a day, she was not eating three meals a day. The
112
— Clinical Applications
therapist pointed out that she was entitled to eat three meals a day, and if she didn’t eat what she wanted at one meal then in a few hours she would have an opportunity to eat again. This simple fact seemed to make a difference. She was much less panicked and much more in charge of her eating. Very slowly she began to make the connection between what she weighed and what she ate and that how much and what she ate was a factor in the measurements and weight of her body. , . Heather’s self-analysis of her face varied from feeling it was “good” to “OK.” At times she would note its expressive quality, like being “tired” or “drawn.” By the twelfth session she begins to observe herself on a deeper level. She says, “I feel transparent, vulnerable, doesn’t look that way. Contradiction between what I’m seeing in the mirror and feeling.” , -. At the beginning Heather’s comments centered around wanting to weigh less. Gradually, she was able to observe the difference between what she saw in the mirror, the objective information she received through what she weighed, and what her measurements were. It was a slow, very subtle process. She faces her phantoms and the reality of her anger and finally says, “I am getting used to it” (session 24). “I just keep telling myself that I’m still underweight and not fat and try to accept the weight.” ₍₎. Though Heather’s estimates were fairly accurate in the linear dimensions, they were about one-half the size in the measurements of circumference. It was helpful for her to see her exact size. It gave her an objective method of holding her size constant in a structure related to reality. She felt this was useful in helping her see that the various parts of her body were in proportion. This was a reassuring revelation. Her fear that she was “going crazy” was dispelled through these very simple and basic tasks. They were helping her to assess her body as a physical sign—the first step in approaching the more complex process of symbolization. Nonphenomenal Tasks
₍₎. Heather’s problem of self-concept is revealed in this, the first task. She draws the members of her family and,
Clinical Applications — 113
though she assigns a place for herself by labeling the space with her name, she does not give herself a line. She says that she does not have a color. She calls this drawing “Sticks.” Because Heather was in a very depressed state, the therapist did not analyze this drawing in depth with her at the time it was made. In looking at the composition of the first CFLD, it is apparent that she felt that she did not belong in the family. Yet, by placing her name in the lineup of members, she indicates her conflict. In assigning the various colors, she tells the therapist that she thinks of people in colors, but that she doesn’t have one for herself yet (see figure 5.20 for Heather’s first CFLD). The second CFLD is nearly centered, with each of the family members given a color, herself, now included, with a green line. The entire group is contained in a mandalalike circle, labeled in black. She titles it “Sunshine Family” and a second label, “The Total.” Heather has always felt it to be difficult to be separated from her family. In discussing this she admits that her former boyfriend was like her father in that he took care
Figure 5.20 —
Heather Allen: First Chromatic Family Line Drawing
114
— Clinical Applications
of her, seeing that she ate and when she ate; he was, in effect, both a surrogate father and mother. In the second CFLD she assigns the same color to herself and her father, both green. ⁄ ⁄ ⁄ ⁄ ₍₎. Heather had a great deal of difficulty executing this task. In her first HTPPA pencil series, both the male and female figures are incomplete, no hands or feet, and the body boundaries are also incomplete. The first chromatic HTPPA is more expressive. She titles the chromatic female figure, “Doll or Little Girl” and responds to the postinterrogation. She says: A girl—no age—a child. She’s standing there looking pretty. She’s fixed, not messed up. Everything’s in place. Looks like a robot, puppetlike. Weighs five pounds, if she’s a doll, [that’s] heavy for a doll. Doll is in a glass case. Nothing bad ever happens. I think of it in a glass bell, protected. She needs a hug. A doll doesn’t have to do anything. Nothing is expected, except always being there and being in place. No opinions. It doesn’t have an opinion. In my house I don’t have an opinion.
Because she was not ready, the therapist did not explore the dynamics of these statements with Heather at the time they were made. Heather cried after completion of the first series of the HTPPA. She explained why she had difficulty in doing the task. She has always felt fearful about drawing. Although it is something she loves, she was never allowed to draw, although it was a field she wished to enter professionally. Her mother would not give her permission to study fine arts in college because it would mean that she would have had to attend art classes where live models posed in the nude. Heather therefore studied in an applied art field but never satisfied her desire to train in the fine arts. The first chromatic animal drawing, which she titles “Jonathon,” is a reference to a popular book, Jonathon Livingstone Seagull. The drawing shows a blue gull high on the page. It has a yellow middle; it is otherwise an empty, expressionless shape. Like the human figures, it is incompletely drawn, openings are seen in the boundaries of the body. The bird is floating on the page with no other reference point. Of this drawing she says: This is a young adult male animal, flying on the beach, trying to fly over the cliffs—he will make it. It’s going to get hurt, going to fall or run into a
Clinical Applications — 115
rock because he’s going to do something that’s impossible for him, go higher than he’s supposed to.
She continues: He wanted to fly. “It’s only with the heart that one can see rightly. Everything else is invisible to the eye.” I feel related to this. My teacher told me I couldn’t do it [succeed in career] and also my mother told me I couldn’t make it.
In the second series HTPPA Heather was still struggling to produce a human being. After many efforts she produced for her chromatic female figure, a picture reminiscent of the wooden, jointed models used in art classes to help the student learn how to proportion the human figure correctly. The drawings in this series lack expressive qualities and substance. While she does manage to create a whole person, she, like the art student, is still trying to “get it right.” Heather’s animal chromatic drawing in this series is a large butterfly, which takes up most of the page. It is depicted as a butterfly on display. The whole range of colors is used, including black and red. She emerges from the incomplete seagull. Of the seagull she says, “Seagulls are near people, eat garbage.” She questions herself: “Does she strive to fly higher, be an eagle, or be a seagull? Maybe it is midway, a robin in the trees.” The butterfly is an expression of hope, transcendence, and rebirth. It is more strongly and completely rendered than her other drawings. Of this she says, “It is fragile-strong, a female in flight.” Heather’s tree in this series is titled “Sunlit Tree.” It is more completely realized than the others, made up of a series of lines that describe its outline; it gives a feeling of strength and solidarity. She acknowledges her animus. She says, “It is an oak tree. I hate to say this: both the trunk and the base are more manly and the leaves and branches are more feminine.” (See figure 5.21 for a photograph of Heather’s second series chromatic tree.) Fearful for a long time to acknowledge her sexuality, she says: In the past, it was horrible, horrendous. I would never have a child. I could never imagine being pregnant and really having my stomach stick out for nine months. How awful! How miserable! How uncomfortable! How gross! How disgusting! But there have been fleeting moments of “Gosh,
116
— Clinical Applications
Figure 5.21
—
Heather Allen: Second Chromatic Tree from HTPPA
it would be nice to have a child.” It’s insignificant, the stomach sticking out. The weight gain, it’s necessary, it would not be awful.
In summary, the first HTPPA series portrays a person operating at a diminished level. Many of the drawings in the second series also define a person who has difficulties expressing herself and allowing herself to exist.
Clinical Applications — 117
But the comparison must be made from herself to herself, over time. In this respect, there is definitely progress. Her chromatic tree is more than the person and the chromatic series as a whole is better than the pencil, indicating that the prognosis is hopeful (Hammer 1958). . Heather’s depression is evident in her first Self Image drawing. It is a black image; the entire circle is filled in with black magic marker. At the very bottom is a small caricature of a head and eyes peeking out. She titles it “Well-Rounded.” She says: “I feel I’m drowning. I feel like shit on the inside, depressed. I feel ugly, unattractive.” Shortly after this she takes an excess of Valium in a suicidal gesture. Fortunately, she calls her girlfriend and mother and they talk her through the crisis. The drawing is an index to her state of mind. Seven weeks later she does a second Self Image. It is bright and glowing, and includes all the colors except black. She calls it “My Color” and says of this: All together. They have to be all together to make up the rainbow. It is a hopeful sign. I don’t want to hurt myself anymore. I’m starting to think of myself as all colors. It’s alive—not dead like the first Mandala.
Heather’s first Body Image depicts her confusion about herself as a physical body in space. This is a drawing in black magic marker of four stick figures, three with large pot bellies, on a strange landscape. Again, it is as if she cannot “make it right.” The second Body Image Mandala, done two months later, shows a single figure filling the circle. It is a pathetic body image, yet it is an improvement over the first, which shows multiple images. Though it is devoid of vitality, sexuality, and is cartoonlike in execution, it is at least a single figure, and it has the concept of a body boundary. The figure, outlined in black magic marker, is inside the circle. Red defines the circle, drawn over the original pencil outline. At this session she is depressed and hysterical over the final breakup with her boyfriend. She gets in touch with her rage: I should be angry that he disturbed my life like this. I have been angry that he wasn’t enough of a person to say something then and do something about it. I always tried to fix it. . . . [He] was weaker than I was, in many ways, and he tried to keep me dependent.
118
— Clinical Applications
She makes an important connection. For the first time she recognizes that he replaced her family, embodying the roles of both her mother and father. In this session she begins to accept herself as a person in her own right. A new freedom is attained. She says: Time passes differently now. The food is not controlling the time. . . . I feel a freedom that I can do what I want to now. I feel steadier—I’m radiating . . . more permanent . . . more stable. I seem more together.
The Body Image Mandala reflects this state. It is surely unfinished, but it is stable and whole. It is a beginning. (For a comparison of the Heather’s first and second Body Image Mandalas, see figure 5.22.) ₍₎. Heather’s first SB, made at the tenth session, is titled “Openended.” She selected a narrow, plain brown liquor box. On the outside she pasted small pictures, mostly in black and white. The words “Efficiency Expert” and “Intelligencer” are pasted on the outside. A toy plush lion threatens a man who has a cartoonlike face. There are many other images, including a man cooking dinner, but the collage lacks integration and appeal. Inside are many pictures, which Heather pasted with great difficulty along the narrow, inner walls of the box. Deep in the box on the back cover is a small picture of a single gravestone in a deserted field. A few dead flowers are draped over the top of the stone. In the distance are some visitors. The flap at the top of the box has no closure. A little way down on one side is a picture of what appears to be a mother and father fighting over a little girl who is in the middle between them. Of the first SB Heather says, “[The] person on the outside looks fine, looks cute on the outside. I don’t feel that way inside.” Heather’s second SB, made six weeks later, is called, “Heather-GoLightly.” It is a large, sky-blue box from Tiffany’s. On the top of the outside of this box a young woman close in age to Heather appears. She is in a bathing suit, painting a picture. The words “Her Life is in Apple Pie Order” appear nearby. On the other side of the top of the box is a modern sculpture. Words appear below it, “Inspired by Life.” The word “Time” and a number of watches are pasted both in and outside the box. Inside, the Statue of Liberty in a Fourth of July fireworks
Clinical Applications — 119
Figure 5.22 —
Heather Allen: Body Image Mandala Comparison of first (top) and second (bottom)
120
— Clinical Applications
display is pasted. The inside of this box is a lot less crowded than the first SB, giving Heather more room to breathe. Heather says: I don’t have to be with someone to make me feel worthwhile. I feel worthwhile just by my own self. I almost felt voluptuous today [122 pounds]. I feel good. I didn’t feel bony. I almost felt kind of sexy. It didn’t bother me that my stomach wasn’t caving in.
₍₎. Heather’s first SW has some elements that confirm her depressed state: a skeleton, a cannon, a stone wall appear and a TV character, the Cookie Monster, is placed in the center. Other items are a boxer, animals that she places behind a stone wall, and a car she said “was always an escape.” The first scene is disorganized and without a theme. Heather’s second SW shows a significant change in her ability to organize and focus. She discusses her second SW: This time I wanted to pick all the pretty pieces, I didn’t grow up on the water, but I love the water. I like the glass—just wanted the pretty things. I like the green, the center is a resting place for the turtles. They are coming in the same direction. I didn’t put it in the center exactly because it didn’t have to be dead center. You can be off-center, centered.
₍₎. Heather’s first KFCS depicts a childhood scene at twelve years of age with her family on vacation at the beach. She is lying down. She says of the first scene: It was hard for me to leave home. I couldn’t imagine what it was like to be separate. I always thought my family was perfect. I used to think that over and over. We never fought and we never argued.
In the second KFCS, done three weeks later, Heather creates a scene at the beach as in the first, but this time she is alone and she is sitting up. She says: Here I am at the beach, was very significant in that I’m sitting up. When you lie down, your stomach sinks in and I’m sitting up and not worrying. There is a towel with a Coke and a sandwich. I will have my lunch. I feel very good, secure, not vacillating. A base, a foundation. I never felt this way before—confident.
Clinical Applications — 121
Combined Phenomenal and Nonphenomenal Task
₍₎. Heather’s first BCD is her most complete drawing up to this point. The figure is standing barefoot and with her feet slightly pigeon-toed. Her hair is held out of her eyes with a barrette. Vertical stripes define the blouse. The midsection is drawn with a yoke and a belt girdling her pelvic area. Her neck is overly emphasized. She discusses the BCD: Looks like she’s standing very rigid. She looks thin, slender. It surprises me, a lot. I don’t think of myself [like] that. She hurts herself by what she puts into her body—by eating and not eating. She’s fine just the way she is I found out a week ago. I’m envisioning how it would be to talk to this person. I care about her. She’s the only one I’ve got, in the end.
The second BCD, drawn three months later, appears more mature and alive. She is standing straight, broad horizontal stripes march down the length of the dress, clearly defining the body. The hair is darkened and framing the face, the features are clearly defined. The body is more alive, the eyes have pupils. Heather comments on the drawing, “She looks real, intense, not angry, fragile, changeable, flexible, decisive, extremely decisive. It’s denied itself for so long. She’s a good friend.” Later, she says, “She looks a little like my mother.” Heather decides to return to the area of the country nearer to where she grew up to be closer to her family and her friends. She makes the decision to look for a job in a city within a reasonable distance from her parents’ home. She also notes that both parents are ill, and she feels it would be good to be closer to them. She finds New York a difficult city to live in, although she has done well in her career, getting a significant promotion during the course of the project. In comparing the two BCDs she says: The old one is childlike, hollow. Looks ten years younger, looks like a doll. The new one has more dimension, looks older, has more depth, not just detail. Head is definitely on its shoulders. Has a focus in the eyes. The toes are indicated. Shoulders and upper arms are rounded and have a strength to them. Spent more time on this one. Has no bow in hair, looks more like a person.
122
— Clinical Applications
(For a comparison of Heather’s first and second Body Contour Drawings, see figure 5.23.) Self Report
. See appendix 1c for Heather’s discussion of her reaction to participating in the study.
Figure 5.23 —
Heather Allen: Body Contour Drawing Comparison of first (left) and second (right)
Clinical Applications — 123
. See table 5.4 for comparison of Heather’s answers to a series of questions in her first and second Eating Questionnaires. Discussion
Heather’s problem was so entrenched, she was so fearful of giving it up, that it was necessary to use the tasks initially as a means to release some of the repressed material without creating anxiety by talking about it. In her assessment of the process she stated that “art therapy works slowly; it’s not magic, it’s gradual.” She emphasizes that doing it slowly, repeating it: “Time after time makes it work—consistency.” In a sense, the tasks were asking her to do the same thing each time, i.e., to respond to ways of looking at herself physically and symbolically. Heather had never had a grasp of her most essential being and needed to get in touch with her body, initially in the most basic way, much as a child first does in learning the different parts of the body and its boundaries by feeling them and seeing ever so slowly where they were and how they work. Heather needed to do this before she would be able to symbolize them. These simple acts were very emotional experiences for her. For so long she had shut herself off from her most basic properties, they ultimately became inaccessible to her. She denied her feeling of hunger. Hunger became pain. Pain became the penalty for the guilt of longing for her most basic needs. She became confused on many levels, sinking further and further into depression and immobility. Living is not worthwhile and she makes the suicidal gesture. There was a split between her life as a competent, award-winning professional and as an inadequate and childlike member of her family. She swung back and forth between them. She could not understand that they were both separate and yet a unity within her. She reconciles these two aspects of herself. She says, I don’t have to explain myself all the time.” She learns how much space she actually is, where her body boundaries begin and end. It is a revelation. She says: The Contour Drawing: I understand for the first time that was exactly what I looked like. That was exactly how much space I took up and it wasn’t that frightening. . . . You can’t deny it. The mirror is not the same. The drawing is like meeting someone, like actually walking up to someone and standing in front of them.
124
— Clinical Applications
Table 5.4
—
Heather Allen: Comparison of Responses to Eating Questionnaire
Question
Answer 1
Answer 2
What is your eating problem?
I’m afraid of gaining weight. I eat better than I used to, but am horrified of weighing more because of it.
Understanding that I have to be a certain weight just to exist is the conflict I’m dealing with now. Realizing that I take up a certain amount of space—I’m trying to understand this.
Do you consider yourself to be a fat person? Why?
Yes.
No.
Because my stomach sticks out.
Because I am still underweight for my height, age, etc.
Do you consider yourself to be a thin person? Why?
No.
Yes.
My stomach sticks out too far.
Because I am slender, I am still underweight.
Have you ever been fat?
Yes.
No
Give weight.
130 pounds.
Discuss this.
I feel ugly, worthless.
Whom do you admire who is thin?
People I see in the office, on the street.
Me.
How much would you like to weigh?
115 pounds.
120 pounds.
What size clothing would you like to be able to wear?
6–8.
9–10.
What is your best asset?
My hair.
My height. My personality.
What goal in your life would you like achieve?
Be smarter.
Just being a good person.
What is the meaning of this experience in this program for you?
I want to get over my fear of food.
Coming to accept myself.
Clinical Applications — 125
Like the developing awareness of the emerging infant, the “gray mists” that had enveloped her begin to dispel, and she becomes conscious of the unconscious forces that possessed her. She recognizes that her boyfriend was a substitute for her family who treated her like a child, which she encouraged. This reinforced dependence. She makes the connection between her mother’s fears related to her own sexuality and how that contributed to Heather’s own confusion and guilt in this area. She has made a start, giving herself permission to live. The multiple body image is reconciled and becomes a single unit. She acknowledges her genetic form and says, “I see that I am in proportion.” Her decision to work in a city near her family does not eliminate the need to separate psychologically from the family nest. Living a great physical distance away only served to isolate her and created a longing for contact. By returning and facing the family from time to time in a natural way, she may be enabled to establish her credibility as an independent adult, long overdue. Nine months after completing the project, Heather writes to the therapist: I know I’ve written this letter to you a million times in my head and never got it down on paper. There’s so much to tell you. First, the very first thing to say is that I’m eating like a normal, hungry person and enjoying every minute of it. My weight remains 123–125. It’s amazing and such a relief. Like being out of prison. I’m still conscious of my stomach, but it doesn’t keep me from those three meals a day! . . . I met a wonderful guy that I’m now engaged to! . . . The difficult part with mother came with not accepting our relationship. I just keep reminding myself that I’m not a bad person and try to ignore the things she says. . . . I even toy with thoughts of helping other people with eating problems because it feels so good to be free.
Summary
1. The TSCS results show increased scores in her overall Positive total, Self Satisfaction, Physical Self, Personal Self, Family, Self, Social Self and a decrease in Variability, indicating a less compartmentalized view from item to item, a more favorable result. These items were duplicated in her art productions. The pictures reflect a better self-view, more flexibility, sexuality, maturation, and positive feelings.
— Clinical Applications
126
2. Answers to the Eating Questionaire were more positive from the first to the second; her estimate of her body as “fat” in the first questionnaire changes to “thin” in the second, a more realistic response, and she recognizes and accepts herself in the Body Contour Drawing, which she says is “like meeting someone . . . it’s me.” 3. In the art work there is aesthetic as well as psychological positive change. Though the pictures do not easily yield to this assessment, an evaluation of improvement must be viewed in the context of her earlier work. There is more significant form, better use of color, and more positive expression. 4. There is a correlation between the verbal aspects, i.e., her gains in the TSCS scores, the changes in the Eating Questionnaire and the Self Reports, which show positive feelings and higher self-esteem. The Self Figures (Body Image, Self Image, Mandalas, and especially the Body Contour Drawing) are more expressive and show growth and maturation. Throughout a theme is repeated: there is a push toward a sense of self. Like the child learning to walk, her surprise and joy in beginning to step out on her own are expressed over and over. She says, “The most fun is to live.”
Linda Miller Tennessee Self Concept Scale (TSCS) Data Analysis
Linda’s Self Criticism Score (SC), 34 in the pretest, rises to 42 in the posttest, and increase from the 48th to the 80th percentile, a gain of 32 percentile units. Her Total Positive Score (P) is 364 in the pretest, and 368 posttest, a gain from the 68th to the 71st percentile. There is considerable discrepancy between her impressive gains in the SC reading and the negligible rise in her overall P score. Her high SC score does not give credence to and support her high P score. The element of defensiveness may account for the inconsistency in these scores. While Linda’s overall P score showed only a moderate gain posttest, there was a considerable positive inner shift from the pretest results to the posttest readings among the variables of special interest to the study. Notable are the positive gains in Self Satisfaction scores from the 74th to the 80th percentile, in Physical Self scores from the 42d to the 70th per-
Clinical Applications — 127
centile, and in Moral-Ethical Self scores from the 74th percentile in the pretest to the 95th percentile in the posttest. Variability (V) increased overall, a somewhat less favorable result, indicating a continuing compartmentalized self-view. (See the discussion section of this case study report for notes on Marazzi and Luby’s [1986] theory of autoaddiction in anorexia.) The final score, Distribution (D), rises from 129 in the pretest to 151 in the posttest. This gain, at the end of the project, indicates a more secure feeling about herself than at the start of the project. Her verbal Self Reports confirm this assessment. Similar changes may be seen in her drawings, which progress from poorly defined and vague boundaries to expressions that are more definite and contained (see figures 5.25 and 5.26). In summary, while Linda’s overall P score showed a moderate increase, more significant internal gains occurred in the variables of special interest to the study. See figure 5.24 for comparison of results of her first and second TSCS. At the outset of the study, Linda stated her problem: I weigh 105 to 106 pounds and I would like to weigh 100 to 102 pounds. Some days I think about food all day. It’s gotten worse over the last year. It’s beginning to interfere with my job. I absent myself from my desk several times a day for fifteen minutes, looking for food. When I leave my desk I go to this fellow who gives me something sweet. Candy. He’s unmarried— I think he’s beginning to make a pass at me. Something psychological prevents me from gaining weight. I’m just afraid the weight will go up and never come down. I don’t understand why I feel this way. I look good and am happy at 102 and am unhappy at 105. I think that’s crazy—that’s why I’m here.
At entrance to the program Linda, who is 5 feet 3 inches and of medium body frame, weighed 104 pounds. According to the Metropolitan Life Insurance weight tables, this was between 17 and 30 pounds under the recommended weight for her height and body frame. Linda is a forty-six-year-old white woman with short, dyed blond hair and blue eyes. She wears eyeglasses. She dressed conservatively in undistinguished outfits. Usually, the dress or pants were tightly fitted to her figure, especially at the waist. Her large hands, size 8½ glove, and large feet, size 9 shoe, made her size 4 figure seem out of proportion. There was a disparity in her manner of
Raw Scores
368
132
131
114 118
118 119
71 76
76 83
65 65
81 79
71 65
54
46
28
27
19 26
129 151
Pretest Posttest
T —95 — — — — —90 — — — — —85 — — — — —80 — — — — —75 — — — — —70 — — — — —65 — — — — —60 — — — — —55 — — — — —50 — — — — —45 — — — — —40 — — — — —35 — — — — —30 — — — — —25 — — — — —20 — — — — —15 — — — — —10 — — — — —5
by permission of the publisher, Western Psychological Services, 12031 Wilshire Boulevard, Los Angeles, CA 90025.
Answer-Profile Sheet (W-182B) copyright © 1964 by William H. Fitts. Reprinted from the Tennessee Self Concept Scale
Linda Miller: Comparison of Results of First and Second Tennessee Self Concept Scale
364
34
42
0.01
LINDA MILLER
0.01
1
0.1
5
5
0.1
10
10
1
20
20
Tennessee Self Concept Scale Pretest (12 Min.) Posttest (10 Min.)
70 60 50 40 30
Percentile
80
D
70 60 50 40 30
Row Total V
80
Column Total V
95 90
Total V
VARIABILITY
95 90
Column E Social Self
99
Column B Column C Column A MoralPersonal Column D Physical Self Ethical Self Self Family Self
99
Row 3 Behavior
POSITIVE SCORES
99.9
Row 2 Self Satisfaction
99.99
Row 1 Identity
99.9
Total Positive
99.99
Percentile
Self Criticism
Figure 5.24 —
95— — — — — 90— — — — — 85— — — — — 80— — — — — 75— — — — — 70— — — — — 65— — — — — 60— — — — — 55— — — — — 50— — — — — 45— — — — — 40— — — — — 35— — — — — 30— — — — — 25— — — — — 20— — — — — 15— — — — — 10— — — — — 5—
T
Clinical Applications — 129
dressing: her clothes were rather little girlish, making her appear out-ofdate and unfashionable. . Linda was born in New York, where she has lived most of her life. She holds a master’s degree in a professional field and has been employed for fifteen years in a nationally known company. She has an appointment in a low-echelon, administrative position working in a job other than the one she studied for. She is unmarried but has been in a ten-year intimate relationship with a man, John, who is married and has two grown children. John lives with his wife who, during the course of the project, suffered a moderately severe heart attack. Linda and John manage to spend weekends together and, occasionally, a vacation. Except for a few woman friends, she has no other close relationships. . Linda’s weight has been down to 98 pounds and, at one point, as high as 155 pounds. She feels her most comfortable weight is 102 pounds. At twenty-five years of age she weighed 130 pounds, and at thirty-five 103 pounds. She uses her own method of weight control, which consists of exercise—mainly swimming—and caloric restriction. She limits her basic diet to chicken, vegetables, fish, and other low-fat foods. She eats a great deal of lettuce and other raw vegetables, nibbling all day. She does not consume any red meat or have dessert at meals. Though she restricts her meals to these items, at other times during the day she will eat candy, but only if given to her by others, and go on binges indulging in a lot of ice cream. She finds the nights after work are the most difficult. She reports getting up at night to eat in the classic, nighteating syndrome (Hinsie and Campbell 1970). Though she feels her thighs and arms are too thin, she doesn’t want to put on weight because “it doesn’t go where I want it to.” She uses food as a reward or to avoid doing something. She says, “If it’s there, I have to finish it, like a compulsion.” Linda did not have a personal physician, she relied on her company doctor for the required annual medical evaluation. This physician responded to the therapist’s medical inquiry. He describes Linda’s problem as “self-imposed dieting and marked physical activity.” He recommended to her that she increase her food intake, which, he notes, she “accepted with reluctance.” He reported that she was gaining weight very slowly. He concluded that she “has a psychologically determined fear of gaining
130
— Clinical Applications
weight.” Linda was referred by the company doctor to an endocrinologist. At that time there was “no evidence of a persistent endocrine abnormality.” In a subsequent finding, however, at a follow-up session with the therapist, Linda reported that there was a diagnosis of a dysfunction of her hypothalamus. . At twenty years of age Linda had an abortion. This coincides with the time in her life when her father deserted the family. She has never told anyone in her family about the abortion. At thirty-four she had an operation to correct Stein/Leventhal Syndrome, in which a wedge-shaped piece of ovary was removed. She has not had a menstrual period since that time. Of this she says, “I really don’t need to menstruate. Am I denying my sexuality?” After this operation her weight dropped to 102 pounds. At forty-two Linda had plastic surgery on her nose for cosmetic reasons and is pleased with the outcome. She has arthritis and Raynaud’s disease. Linda has not been in treatment for psychological problems before participation in the project. . Linda’s mother is seventy-six years old and a widow. She has had her uterus removed, otherwise no other medical problems reported. She is very active and continues with her hobby of square dancing. Linda says of her mother, “She’s indestructible.” Linda maintains close contact with her mother and, although she does not live nearby, continues to visit her regularly. Linda remarks, “She knows how to put the needle in and put you on a guilt trip.” Linda’s father was a physician. He had a heart attack when Linda was fourteen years old. At that time the family, all of whom were overweight, changed their eating habits so that the father could lose weight. Her father was in the U.S. military service for three and a half years. During that time the family traveled with him, living in different cities. Linda attended seven different schools through this period and as a result was unable to establish long-term relationships with her peers. When Linda was twenty her father left her mother and subsequently obtained a divorce without telling his wife. He remarried one year later and moved south. Linda never saw her father again. Although she wanted to visit, her father did not permit her to do so. His behavior became erratic
Clinical Applications — 131
and unpredictable and Linda grew more attached to her mother. She says, “I was probably very sympathetic with my mother.” She was upset at her father’s behavior and as a result became angry and detached from him; she was not in contact with him during his last years. He died a few years after remarrying, leaving all his assets to his new wife. Since that time Linda has denied her former attachment for her father, which had been considerable. Though she was always considered to be her “mother’s daughter,” and her sister was her “father’s child,” she always felt a special closeness to him; he respected her abilities and encouraged her to pursue a professional career. Linda’s only sister is two years her junior. At nineteen the sister had an abortion. She is divorced and has two children. At the outset of the project Linda’s relationship with her was formal and maintained only because of family events, such as her nephew’s wedding. Linda was critical of her sister’s lifestyle, which is to portray herself openly as much younger than she actually is. She was currently having an affair with a much younger man. Linda describes her sister as “an artist who is overweight, doesn’t know how to manage her funds, and is constantly on a diet to lose weight.” She characterizes her sister as a ‘’fifty-year-old immature grandmother who pretends she is thirty and is vain and flashy.” At his death her father’s body was brought north by his second wife and buried in New York, but Linda had never visited his grave. Six weeks into the study, at Linda’s suggestion, she and her sister visit the cemetery where he is buried and spend a tender three hours together at his gravesite. During this cemetery visit Linda and her sister reestablish their relationship, which had been aborted since the death of their father. Their good feelings for each other increase with time. Linda counts this as a significant outcome of her participation in the study. Project Compliance
Linda was very willing to participate in the sessions, but work commitments out of town extended the periods of time needed to complete the tasks. She did each task as requested, but did not volunteer any conversation unless it was initiated through the work. Doing the task and analysis seemed to release many memories and associations for Linda and served as a valuable means for her to get in touch with her feelings, which
132
— Clinical Applications
she normally kept constrained. She began to have rich dreams, which she shared with the therapist. As she became more experienced in analyzing her art productions, she was able to understand some of the dream content as well. Linda discussed the art therapy experience: I have found this whole experience amazing because I am . . . noncommunicative. . . . I don’t say things very often. What’s coming out of the drawings has been more of an expression of how I really feel. . . . This to me is fascinating. . . . It’s almost unbelievable that . . . things can come out by drawing as opposed to speaking especially from somebody who considered herself a lousy artist. . . . I don’t think it could have been expressed any better in words.
Phenomenal Tasks
. Though Linda’s problem was focused on her fear of gaining weight, she was willing to be weighed each time. Seven months after the start of the project, she talks about the process: It’s good for me because I tend to think I’m overweight, so I will not [choose to] get on the scale. . . . So by having to get on . . . once a week, puts me back in perspective. Where some days . . . I imagine I weigh 120 pounds, and I only weight 104. I say it’s not so bad.
Linda’s weight in twelve months varied from 104 pounds at entrance to the program to a high of 106 pounds and a low of 101. Her general health was good throughout. , . Linda’s response to viewing her face was always dispassionate. She rarely had a strong emotional reaction to anything. Certainly, at the beginning, she viewed her face as that of a stranger and, without affect, she says, “I see creases in my face, the arms and a short skirt, bell-shaped legs.” Generally, she felt she was in good shape. It was only in analyzing the art work that any feelings were released. , -. Linda’s response to viewing herself in the full-length mirror was also very restrained and bland. She tolerated looking in the mirror but was unresponsive and seemed disinterested in what she was seeing.
Clinical Applications — 133
₍₎. Linda estimates her shoulder to be 8 inches; in reality it is 3½ inches. She underestimates the dimension of the roundness of her head. Perhaps an index to her conflicted feeling of wishing to be very powerful, i.e., having broad shoulders and, at the same time, feeling that she is not intellectually capable of performing at a high level, i.e., having a good-sized brain. Nonphenomenal Tasks
₍₎. Her first CFLD shows Linda’s entire family, although none of them live together; she includes her father as well, who has been dead for the last twenty years. Of the drawing she says, “I made myself fatter. I selected blue for me because that’s my favorite color. Pink [her mother’s color] is vivacious, and my mother is terrific. Orange [sister’s color]—don’t like that color, almost gaudy.” Then she observes, “I made my father blue—blue is for boys.” She muses, “I would have liked to have a brother.” She does not make the connection between her color and her father’s (both blue), nor the fact that she says (in effect, about her own color), “Blue is for boys.” Linda here recognizes her longing for her father and discusses his desertion of the family. Though she is angry with him, she realizes that he was a significant person in her life who cared about her, and she about him. In spite of her mother’s expressed hatred for him, Linda acknowledges that she does not hate her father but only pretended to because she did not want to be disloyal to her mother. In the second CFLD, done two months later, both she and her father still have blue as their color, but Linda’s blue is now a different hue from her father’s blue. Linda now adds her new color to her father’s line, and moves her self line closer to her sister’s. The mother is now distanced from all, taking Linda’s former position. The sister is now given a double line, indicating Linda’s increased understanding and feeling of closeness to her sister. Linda’s self line is now slender, and her mother’s line is a double one, open in midsection, perhaps an expression of Linda’s admission of the dual nature of her mother as both “terrific” and one who “knows how to put the needle in.” ⁄ ⁄ ⁄ ⁄ ₍₎. In Linda’s first series HTPPA the lines generally are faint and the features in the human figures are
134
— Clinical Applications
vague and amorphous. The boundaries of the figures are pale and incompletely drawn. There were many erasures and much resistance to doing the first series. After the five pencil drawings, at the request to do the chromatic, Linda says, “If she [the therapist] thinks she’ll get a different house out of me, she’s crazy!” She outlines the house in red crayon, perhaps as an expression of her anger. She may have felt controlled, much as she feels about her mother or her boss, with whom she was having difficulties. By the time she does the first chromatic series, she has become less defensive. She draws the female figure and recalls a memory of an affair with the man whom she portrays in the second figure drawing. She became pregnant with his child and secretly had an abortion, which she has never revealed to her mother. Later she relates her mother’s reaction to learning of her sister’s abortion, in which the mother said “I hope it was worth it.” Her first series HTPPA takes sixteen minutes, the second series, done eight months later, takes forty-eight minutes. She was more willing and more attentive and less afraid of her feelings. Of the tree drawing, she comments, “It needs a wider base. There are no houses nearby.” The image of the blue spruce in her first series is described by Linda: “As I get older and colder, I like a tree that represents winter, evergreen.” In her second female figure drawing, eyes (which do not appear in the first) are depicted. The figure has more substance and the body boundaries are defined. The face is more clearly drawn and the hands are visible and more natural. The female figure is in better proportion; shoulders are drawn a little narrower and reflect a more realistic physical dimension. The animal she selects in all four animal drawings is the pet dog she had as a child. Linda says, “When he died, I cut off something, didn’t want to believe it.” In some ways her reaction to her beloved dog’s death was a scenario she used over and over in her life. By not attending her father’s funeral and never visiting his gravesite, and by her continuing relationship with her married boyfriend John, she is denying certain real events that have occurred in her life. She continues to include her father in her depiction of her family, although he has been dead for twenty years and absent from the family constellation for twenty-five years. At this point
Clinical Applications — 135
the effect on an unconscious level is to perpetuate the myth that the father is still alive or that someday he will return. Soon after completing the HTPPA series she makes an appointment with her sister and initiates the meeting at the cemetery where her father is buried, which neither of the sisters had previously visited. For the first time she shares her intimate personal secrets with her sister, who responds in a sympathetic and positive way. Though Linda does not tell the mother of her abortion and affair, she is now able to be a little more open with her. The cemetery visit marks the beginning of saying “goodbye” to her father. It is a beginning of truth and reality. Linda notes some new feelings; she no longer eats standing up and is paying more attention to the process. She also acknowledges that she would like to have a husband, something she had not allowed herself to admit before. Finally there is illumination. She says, “I keep putting my father in the family and left my mother out.” In summary, the HTPPA shows improvement from the first series to the second. There is a clearing in the structure and integration in the use of color and creation of form. Her ability to express and identify her feelings increased. Awareness of what she is and feels are basic human skills that either she had never acquired through the normal developmental stages as a child or through time had been rendered inaccessible to her. . Linda’s first Self Image Mandala depicts a blue rectangular form, 3 inches by 8 inches and centered in the circle. She labels this form “Boss.” Outside the circle is a small, blue, uneven box, 1 inch by 1 inch. This is labeled “Ghost.” The picture is supposed to represent her relationship with her superior at work and herself. She titles the Mandala “Unacceptable.” In analyzing this drawing she sees that both her boss and herself are in her own (and her father’s) color, blue. The conflict of the concept of her boss as authority, both benign and threatening, is apparent. The Mandala may represent two aspects of herself. She is her own “boss” and, therefore, perhaps self-inhibiting. This idea is not yet available to Linda. At the same session she makes a second attempt to reconcile her conflict and creates a Mandala that she titles “Cooperation.” It is an abstract picture of herself and her boss. She envisions him as the
136
— Clinical Applications
abuser and herself as offering cooperation. However, in the picture it is she who is seen wielding a knifelike object toward him. For the first time she sees her aggression revealed, though contained. Linda now realizes that, although she thinks she is pleasant and controlled, her quiet abhorrence can be seen and felt as hostility by others. She says, “I’m a very angry person. . . . I always rolled with the punches and took everything as it came . . . [I thought it] didn’t really disturb me, but obviously it has.” The second Self Image Mandala, called “Happy Days Are Coming,” features a large sunlike face taking up the whole circle. It has facial features that appear hollow and meaningless, much like the commercial and vacant “sun face” used everywhere as a logo for “Have a Nice Day.” The form is outlined in red magic marker, and orange and red lines emanate from the sun. It is without eyes, nonseeing and vacant, a feelingless form. The title and the picture are incongruent, yet it is a beginning. She dares, in a more integrated way, to use the outside of the circle even though she does not fully comprehend what is going on inside her. She says, “I think we should all know why we’re doing what we’re doing when we’re doing. I’m not as guilty afterwards. I may still be upset and a little angry to be getting at myself, but the guilt doesn’t seem so bad.” Linda’s first Body Image Mandala is called “Friday.” Labels appear inside the circle: “pale,” “yellow,” “neat,” and “color coordinated.” A female figure in pants and shirt appears at the bottom of the circle. The pencil outline is untouched. The body is wide at the hips and looks fatter than herself. It is indeed “pale” and looks as if it is fading away (see figure 5.25, top). Her second Body Image Mandala, done four months later, is called “Control.” The circle is now outlined in Linda’s blue and she appears more like herself in form, performing a difficult feat, i.e., standing upside down on her hands with no support. She is clothed in a green leotard. The body is more natural, breasts are apparent, and her figure is revealed, in contrast to the first drawing, which showed her in loose, baggy clothes. All the labeling is confined to the inside of the circle. She demonstrates that she is in control, but she is obviously in a precarious position and uncertain as to how long she can remain in such a stance. The eyes are intense and the mouth is red with effort or anger. Linda talks about the meaning of control in her life: “I fear things that are beyond my control.” She recognizes that food may be a way of
Clinical Applications — 137
Figure 5.25 —
Linda Miller: Body Image Mandala (top) Self Image Mandala (bottom)
138
— Clinical Applications
assuming control. Her relationship with John is “out of control,” and this makes her angry. She may not be able to hold on much longer to an untenable position. She continues, “Sometimes you almost analyze people you know. You think they’ll do something or make a certain move and they don’t do it and [it] really shocks you. You make an assumption and you’re wrong.” Linda needs time to think about her position on her job and with John. Perhaps they do not have to be solved in the same way. In a follow-up session she reports that she has had a very good job promotion but that the situation with John remains the same, i.e., he is still living with his wife and there is no discussion of divorce. She draws another Self Image Mandala and calls it “Relaxed.” It is a glowing self portrait. A whole person has emerged; one who is alive and appears to have substance. The boundary of the circle is purple, a new color for Linda. It is firm and closed. Linda appears inside the circle, looking out directly into the eyes of the viewer. Her hair has returned to its natural brown, her eyes are focused, her mouth is soft and pink, and there is a suggestion of breasts beneath the blue dress. The figure, filling the circle, is a realistic rendering of herself. It is a beautiful and credible portrait. (See figure 5.25, bottom). In comparing the first Self Image with the most recent, the change in her self-concept is striking. The drawing is integrated, aesthetic, and psychologically more healthy than in any of her previous work. ₍₎. The first SB depicts her conflicts related to food and her body. On the outside of the first SB she pastes a bulldog dressed in a chef’s hat and bib. The dog is seated at a table facing two plates of food, one appears to contain commercial dog food, and the other a thick steak. Linda signs her name directly under this image. Inside the box is a large, life-sized head of a woman eating a tomato, and under this is the sentence “Taste is Everything.” Nearby, is a cartoon rendition of a twoheaded Siamese-twin woman joined at the torso. One half is wearing boxing gloves and appears to be attacking the other half. On the underside of the cover of the box is a young couple. The man is seated; his hands are touching the abdomen of the woman. Their costumes appear to be
Clinical Applications — 139
from another time, perhaps Victorian. There is lace in the background. This scene could represent a memory of her old affair and subsequent abortion. It is the nature of this task that all of the items are cut out of magazines and pasted down in a collage. Linda left a loose silver cord lying inside the box. It is an almost perfect message. Hinsie and Campbell (1970) identify the Silver Cord Syndrome, “A family constellation consisting of a passive or absent father and dominating mother” (p. 743). It is an apt description of Linda’s early life at home and the struggle she is experiencing. The second SB also has a man and a woman, this time on the outside of the box, eating, and a picture of a woman drying her hair. Inside another couple appear, but from a distant view. This scene is a memory of Linda and John on a vacation in Europe together. In comparing the two boxes, she says, “Last time I put the man and woman inside the cover, you couldn’t see it. Now, you open the box and there it is! It’s the only thing I still want in the box, a little more in the open.” She begins to face the reality of her situation and the need to make some hard decisions. ₍₎. This exercise, which uses toys and other concrete forms, is a relief for some of the subjects as it does not require them to create an art work. Linda, however, found it difficult to relate to the items that were presented. (For a description of this task see chapter 4.) Linda discusses her first SW scene: “I didn’t want it to be closed . . . tended to use every corner [yet] left a lot of space.” She includes a scarecrow in her scene. Of this she says, “The scarecrow protects and preserves, keeping the animals away from the food.” The SW figures evoke associations: I think I have this problem in my life . . . be independent and do what I want to do when I want to do it . . . and am also looking for somebody to look up to, somebody to give me advice, to tell me what to do and almost like—this fatherly advice, someone I respect and care for and love and trust. He’s protecting and preserving.
In discussing the meaning of a scarecrow with the therapist, she observes that the scarecrow is dressed in a tie and hat and could be mistaken
140
— Clinical Applications
for a human male figure. She says, “Looks like a male person waving ‘come on.’ ” It is a seductive image. The scarecrow could represent the intimate male authority figures in her life, i.e., her father and her boyfriend. Looked at from a great distance, the scarecrow may fool some animals and some children and perhaps an immature adult, but in reality he is never meant to be real but merely a facade for a person. He is, in fact, symbolically, “a dummy, an image of the soul, in primitive belief, like a doll and any figure that bears a human likeness. Hence the belief in its magic properties” (Cirlot 1971:90). Linda’s continuing fantasy of her having both her dead father and her married and therefore unavailable boyfriend function as living entities in her life is amplified in the SW. She seeks a benign authority to serve her needs, but they are immobilized and dumb to her requests and, because they are dumb, are unresponsive to her needs. She is still fearful of facing reality. She says, “The boss might take another turn and become strict and strong. There’s always that concern.” She attests to the conflict of her wish to be nurtured and dependent and her fear of the control this position engenders. In another area of the first SW there are cotton balls, a harp, and a broken watch showing the internal workings of a clock stopped in time. She relates to this: I don’t really like time constraints. . . . I guess I’d like life to be heaven (laughs), but it certainly is not that way. I’d like it to be easy. I can work hard and I do work hard to get what I want . . . not always so sure what I want. Again, looking at the Sandworlds scene, she says, “Timeless—maybe I’m reaching that age where I’m really wishing I were timeless.”
In the second Sandworlds she says, “Chose some dice and shells and some of the same items as the last time.” She reflects on her situation: “Dice appealed to me today because life is a chance, but we can’t live a good life unless you take a chance, some of which I’m not prepared to do at times and some of which I am.” She affirms that her situation is her choice but is not prepared to face the consequences: “The broken watch still appeals to me in terms of timelessness, not having to keep time and having a schedule . . . doing what you want when you want to do it.”
Clinical Applications — 141
At almost fifty years old, she is facing a life crisis; her biological clock is running out, a theme that was expressed in her Self Boxes. ₍₎. The first KFCS depicts three members of her family, i.e., her father, her sister, and herself. The sisters are holding hands and their backs are toward the father. He is looming over them, his head a grotesque shape. Linda calls this scene “Farewell.” In the scene she is saying goodbye to her father when he left the family. After this task she begins to let her hair grow back to its natural, light brown color. She reports that her eating behavior is somewhat better, i.e., she is not standing up to eat as in the past. She also has a feeling for the first time that she would like to have a husband. She feels that it may be possible for her to establish a permanent relationship with a male. At the next session she brings in a poem she had written in response to these memories of her father. She titles it “Taking Leave”: Taking Leave Now you’re gone Joy no more Emptiness. Life goes on More joy to come Somewhere.
Three months later she does a second KFCS in response to the task to improve the first KFCS. The scene depicts the same figures; this time the three people face each other, forming a small circle. She says: The first one was very detached and cold, unfriendly. I thought I should depict the goodbye with tears and hugs. Tears and hugs were certainly there, not just a wave of the hand. I remember some pleasant times when we did things together. I can picture my father as doing other things as well. I’m sure it was hard for him as well. It’s just a happier scene.
Combined Phenomenal and Nonphenomenal Task
₍₎. In the first rendering of the BCD (see figure 5.26, left). Linda added very few details to the original tracing made by the therapist. Only the waistline is corrected in red. Linda adds a bracelet and sketches hair, which stays inside the drawn outline. Although features
142
— Clinical Applications
Figure 5.26 —
Linda Miller: Body Contour Drawing Comparison of first (left) and second (right)
of the face are drawn, they are very faint, and it is barren and expressionless, made more so by the absence of pupils in the eyes, which appear as empty and vacant holes. Linda’s second rendering of the BCD, done only three months later, shows a marked change in her depiction of her body (see figure 5.26, right). There is a strong emphasis on the body boundaries, especially in the torso area. Heavy lines done in poster paint (a less controlled medium
Clinical Applications — 143
than the original markers) are a bold and courageous effort. Here Linda not only defines the body, which appears to have substance, but includes an indication of breasts. There is much more assurance in the stance and also more expressiveness in the face. Pupils appear in the eyes, which now look out at the viewer. In an effort to realistically portray herself, earrings and lipstick are indicated as well as ample hair. The lips appear softer and less tightly closed. As in the first BCD, the hands and feet are still undefined; her ability to be more effective and reach out to people in the environment was yet to come. In this therapist’s experience the anorectic and the obese are often unable to recognize themselves as the image in the mirror. In this connection Linda states: I was astonished the day we drew me on the wall. I couldn’t believe it was me up there. I thought something was wrong with the mirror. I thought in certain stores when you go to try on clothes, that they almost bought mirrors that make you look a little thinner. . . . People want to look thinner in general. I really thought they bought mirrors that make you look like that.
The BCD makes an impact that the mirror cannot. Though it is twodimensional, showing only length and width, it nevertheless is recognized by Linda as authentic. She reports on this experience: “The Body Contour Drawing was actually me . . . it was drawn to my contour and I believed it. You didn’t cheat.” Linda uses the word actual in referring to the BCD. The mirror is merely an illusion and subject to distortion and is a “virtual” rather than an “actual” image. Gombrich’s (1956) discussion of the mirror image offers a key to this phenomenon. He says: “Illusion is hard to describe or analyze, for though we may be intellectually aware of the fact . . . that any given experience must be an illusion, we cannot, strictly speaking, watch ourselves having an illusion” (pp. 5–6). While some studies (Norris 1984) have used mirror confrontation for self-estimates of body dimension, the studies have not accounted for the fact that the mirror is an illusion one-half actual size. For the individual to “see” himself as he really is, the mirror image requires the subject to make a three-part transition from the phenomenon of the actual body,
144
— Clinical Applications
which may be described as the sign, to the illusion of the body in the mirror, and, finally, to the authentic symbol for the body. This requires the subject to hold constant the genetic body template, though the body size due to weight changes may fluctuate. Susan Langer (1942) discusses symbolic transformation: The essential act of thought is symbolization. . . . Sign-using and signmaking . . . stand forth clearly as the essential means of intellection. . . . Symbolism is the recognized key to that mental life which is characteristically human and above the level of sheer animality. . . . There is a profound difference between using symbols and merely using signs. (p. 29) The passage from the sign-function of a world to its symbolic function is gradual, a result of social organization, an instrument that proves indispensable once it is discovered, and develops through successful use. (p. 32)
The Body Contour Drawing, crude as it is, is based on the tactile experience of having the magic marker, guided by the therapist, touch the subject’s body as the tracing is made. This truthful and phenomenal rendering on paper remains as a permanent record of the individual’s body as it is. The person knows this is truth. (See the description of the BCD method in chapter 4). This experience secures for the individual the body as a bounded object in space and attests to at least two dimensions, namely, length and width. Inaccurate body dimension perception is one factor in inappropriate body image perception. Norris (1984) suggests that body dimension accuracy aids in establishing a stable and relative self-concept. It is typical of the subject to be astonished at the BCD. It is, at times, a traumatic event. It is the “sign” for the body, as Langer says, that is, the actual body experienced as the therapist traces around the body. Within the same exercise the BCD becomes a symbolic expression of the body as well when the subject fills in the details and creates a portrait. The tracing uses the actual body; the drawing then becomes a transitional means of symbolization toward constancy of body image. In a single task the BCD and the postdrawing verbal interrogation combine both conscious and unconscious elements of the body.
Clinical Applications — 145
The importance of the individual’s ability to accurately symbolize self-experience is further defined by Rogers (1959), “Thus when self experiences are accurately symbolized, and are included in the self concept in this accurately symbolized form, then the state is one of congruence of self with experience” (p. 206). Self Report
. For an extract of the tape recording in which Linda discusses her participation in the project, see appendix 1d. . For a comparison of Linda Miller’s first and second responses to a series of questions on the Eating Questionnaire, see table 5.5. Discussion
Linda’s overriding problem was her massive denial of her feelings, both positive and negative. She had entered a world of fantasy, and she was depressed and immobilized. She had entertained the idea of suicide. She says (while driving in her car at 60 mph on the highway), “I thought it would be easy to just let go of the wheel.” If she just “lets go of the wheel,” she would not take a direct action, the car might run into a tree, and she would not be responsible. With a weight phobia, amenorrhea for fifteen years, obsessive need to exercise daily, a severely restricted caloric intake, and a weight of 103 pounds, she says, “I’m not anorectic or obese,” even though she answers an ad seeking obese or anorectic subjects for a study. She is not sure of herself, not knowing who she is or where she is. She says, in discussing her SW, “at the pearly gates. I think life should be heaven.” She assigns a scarecrow the place of power at the head of the table, believing this to be appropriate. She remembers her own father in this role. She acts out her childhood scenario in aligning herself with her boyfriend John who is an older, married, family man. She is resigned to seeing him between his family commitments. Though she denies her progress (perhaps as a way to prolong the project), an examination of her own words attests to the fact that positive
146
— Clinical Applications
Table 5.5
—
Linda Miller: Comparison of Responses to Eating Questionnaire
Question
Answer 1
Answer 2
What is your eating problem?
I tend to go on binges, eat a lot of ice cream. I don’t know if it’s a physical need or a psychological problem. I constantly think about food. It’s gotten worse over the last year.
It allows me to eat. I’m not as guilty afterwards. . . . It doesn’t seem so bad. It doesn’t seem to color my whole attitude for the day.
Discuss being thin.
If I weigh 102, I’m happy. If I weigh 105, I’m unhappy. Something prevents me from gaining weight. I’m afraid of getting fat again.
It’s a little crazy to be worried about my weight when I’m this weight (104). If my weight is up (105), I don’t panic, it’s more manageable. I don’t feel the guilt. I can eat a little more.
If you could change one thing in your life, how would you?
I fear things that are beyond my control. If I had been a man, I might have had a different profession or gotten further or been somewhere else.
After a difficult time at work, I handled myself a lot better. Stood up for my rights. Before, I would have backed down.
What is the meaning of this experience for you?
I weigh 105–106 pounds and I would like to weigh 100–102. I’m afraid the weight will go up and never come down.
I discovered that deep down inside I’m a very angry person. I always considered myself calm, cool, and collected. I’m trying to express myself more and I’m trying to eat more normally and more regularly, and I’m talking to myself a lot more when I’m not doing what I’m thinking I’m trying to do.
shifts have occurred in her ability to face reality, to give up her fantasies, and to acquire her memories. She comes to terms with her gross denial of her self-abusive behavior. She expresses surprise at the illumination of her strong feelings. She says, “I discovered that deep down inside I’m a
Clinical Applications — 147
very angry person.” She is able to identify the source of these feelings and titles them as both “Anger” and “Hurt”: Father leaving mother, leaving me, leaving assets to new wife, refusing to let me visit Thanksgiving. Mother sending me on guilt trips. Sister thinking mainly of herself. Commanded father’s affections. John not divorcing wife. Not being able to “go places.” Boss being insensitive to business needs. Myself not being more aggressive. Not being able to control food consumption. Being compulsive about exercise.
She acknowledges her positive feelings for her deceased father and allows herself to express love for him. Her mother admits that she “poisoned (Linda) against men.” Linda says, in drawing and doing the clay, “I kept putting my father in and leaving my mother out. I was mother’s girl. I never talked about men in my life and I never talked about doing other things.” A more open relationship develops with her mother and a more loving and close one with her sister. She admits, It takes a while to sink in. . . . I imagine that five years from now that it is still going to stay with me and that when I’m far away from this [therapy] it’s still going to stay with me, and at times of crisis or problems it will be useful then.
Because Linda’s eating problem had persisted for about twelve years during adulthood, it may have become entrenched and appeared now to be a chronic syndrome. Marrazzi and Luby describe this pattern: Anorexia nervosa may then be understood as a psychobiologic process in which dieting to achieve a prepubertal weight will then initiate a series of central nervous system changes that then perpetuate the disorder and in some instances make it irreversible. An auto-addiction may evolve over time to the pathophysiology of weight loss. Clinicians have long observed that the longer anorexic patterns exist, the more likely it is that the disorder will become irreversible. (Marrazzi and Luby 1986:192; see also Crisp, Kalucy, and Harding 1977; Halmi et al. 1977)
If Marrazzi’s concept is valid, it is unlikely that Linda could achieve total relief. In the project, recognition of the reality of the problem and management of some of her symptoms served to relieve her pattern of guilt and feelings of helplessness and dissipate her depression and anger.
148
— Clinical Applications
In summary, Linda recognized that though she is a physically small person, it is not necessarily an index to her dimension as a total person nor her capacity to make an impact. She understood that she had, by continuing to seek care and nurturing from others,wished to consider herself a younger person and to remain so, physically and emotionally. She became less occupied with the notion that exercise and dieting were the most important things in her life. There was less guilt about eating and better relationships developed with her family. The trip to the cemetery was, in fact, a pilgrimage to bury the past. She was beginning to face the reality of her relationship with her boyfriend. When last seen in follow-up she reported she was now 110 pounds, was pleased about a significant job promotion, and was being treated by an endocrinologist for her metabolic dysfunction. Summary
1. Though Linda’s Total P score in the TSCS did not change by very much, there were significant positive shifts in her score for Physical Body through realignment in the internal scores. She had increased her authentic perception of her body size, sexuality, state of health, physical appearance, and her skills. 2. Linda’s Self Reports show definite improvement in her attitudes about food, weight, family relationships, and work. She reaches an understanding of some of her feelings and allows herself—at least with family and work—to express these feelings. She no longer panics. 3. Linda’s renditions of herself in the Mandalas changed over time. Though she never became totally facile with the art media, she gradually used more and varied media. She advances from the thin magic marker to the bold use of paints (see figure 5.26). In a follow-up Self Image Mandala her increased self-esteem is apparent in her drawing. The pale, faded figure dressed in pants and shirt changes to a vibrant woman (see figure 5.25). Both aesthetic and psychological changes can be observed. The picture is focused and expressive of how the person appears in reality, alive and well. 4. Her progress in her verbal reports and the TSCS, the Eating Questionnaire, and the Self Reports indicate growing awareness and responsiveness to inner messages. There is reflected in her nonverbal work positive
Clinical Applications — 149
changes, more realism and congruence between these two aspects. The female figure drawing, the Mandalas, and the Body Contour Drawing reflect these positive changes. She becomes aware of how she had created a fantasy and was living it. She says: I guess I’d like life to be heaven (laughs), but it certainly is not that way. . . . Maybe I’m reaching that age where I’m really wishing I were timeless. . . . I really feel that I am actually able to express my feelings! Fascinating. Almost unbelievable that this can happen in this way, that things come out in the drawings as opposed to speaking. . . . I have reached a stage when I can say to myself, “You’re small. You’re silly to think this way; you’re silly not to put on a couple of pounds if you feel like putting on a couple of pounds. You’re not going to kill yourself. People will still love you or like you.”
The case studies measure the progress over time of each participant, herself to herself. The pictures comparing the first series of tasks to the second document and validate the process. What emerges from a review of the data is the common reaction of the individuals, both in their pictures and words that echo each other’s perceptions and emotions about their illumination and progress. The process of repeating what was the same issue, i.e., self-concept, over and over, overcame their denial and revealed their truth. None of the participants were together as a group and yet their responses showed similarities that cannot be dismissed as coincidental. At times their words about what happened to them were identical. Their pictures also showed where they were. Butterflies were evident in words and pictures; spontaneous statements about rebirth were also common. For a long time the use of art therapy in traditional research had been considered unattainable because of the difficulty of analyzing pictures in a statistical format. Creativity and intuition, often perceived to be the exclusive domain of the artist, are valid and critical parts of any good research procedure that might employ statistical instruments of measurement. I envision expressive art being accepted as reliable scientific evidence in its own right. Cooperative efforts on the part of the art therapist and the more traditionally oriented researcher can create new and sound means toward accomplishing this goal.
150
— Clinical Applications
The use of the PNBIT could be a base from which two-track investigations proceed in eating disorder units of hospitals, cross-fertilizing medical and art therapy research methodology. Hybrid methods of validation may need to be developed, with results presented and written as a joint project. These efforts would create avenues of information between the medical research community and the art therapist, increasing respect and interest in each other’s work. Medical education has progressed where nutrition courses for medical students are now required as part of the curriculum. Art therapists must also accept the need for verbal communication as vital to successful treatment. The resistance of each has created a difficult political atmosphere and continues to impede validation of art therapy, long overdue, to its rightful professional stature.
CHAPTER 6
Conclusion
Prevention-Intervention: Role of Family and School The airing of information on the hazards and devastation of eating disorder syndromes ebbs and flows. Periodically it goes underground: for the women the return to the closet and for the men, who until recently never came out of the gyms in the first place, remain well hidden. There is no scientific consensus on either the etiology or effective longterm self-management of these insidious syndromes. The forces that impact on the individual who is struggling to identify herself as a unique person are multidimentional. The attempt to remedy the problem by addressing the symptom, whether it is expressed in an eating disorder, alcoholism, gambling, smoking, use of drugs, licit or illicit, excess of spending, sex, or work, is a temporary solution. The addictive process is a fluid one. It’s like pushing a balloon in one spot, and it merely flows to another, unless it is stretched to its limit and explodes. The need to access an authentic self-concept is a preamble to alleviating the destructive symptom and self-managing the expression of the addiction, whatever its manifestation. The emphasis on women as the major group effected with these disorders has limited eating disorder research and treatment programs directed toward males. Art therapy academic curricula encompass a broad —
151
—
152
— Conclusion
scope of study, yet the majority of graduates who become registered art therapists continue to be women. The two issues complement each other. As more men are identified and seek help, it will generate more interest from the medical community to initiate both research and mental health programs for males. This may encourage more men to pursue art therapy as a promising career avenue. Coming full circle, men may feel more comfortable working through their problems of body image with male therapists, at least initially. It would serve women as well to have the option of male or female as therapist. It is hard to reassess physical dimension when this vital ability has been distorted. If a person experiences himself during childhood within his family in a certain role—labeled by father, mother, siblings as fat or stupid or “less” than another—he cannot come to the present, perhaps when he has lost weight and actually looks different—genetic shape restored, etc., because his perceptual apparatus becomes forever enslaved through experiences and “knowing”: we cannot help distorting our perceptions given our knowledge. This may be why a person cannot seem to give up the old ghost of the fat or distasteful person. Once we learn how a thing or person is supposed to be, we experience it differently and never again as directly. Experience places an obscuring veil of understanding between us and the world. We need to puncture that image and come to it childlike—as an artist with fresh eyes. The PNBIT does both—helps the person see herself, purely, with fresh eyes through the manifest content, and then again, deeply, with understanding based on unconscious truth from the latent content. The phenomenal and nonphenomenal tasks provide the person with the tools. The self-concept becomes apparent and gives the individual the courage to explore the past. In the method of looking at the pictures free association plays a role, but the person is given rich concrete dream material to work with. It is evident that early experiences play a role in the healthy development of all individuals. It is no less so for those who are at risk for the advent of addiction. Families attitudes about food and eating impact on the ability of those at risk to develop appropriate patterns of behavior associated with the body and its image.
Conclusion — 153
Some addictive behaviors are related to the abuse of illegal means; few are necessary to sustain life. Because food is both necessary and legal, it may be the most difficult to manage. When the eating disorder becomes life threatening, and the person is in a crisis, drastic measures such as close monitoring within a hospital setting may be used. The offending symptom is moderated and the patient is discharged. Such a scenario may precede a more severe condition. An obese person who has undergone heart surgery is now fearful of the consequences of another episode. But patients’ resolve to follow the prescribed recomendations by their physician to “change their lifestyle” may result in depression for both the anorectic and the obese. The anorectic becomes more secretive in order to continue the goal of restrictive eating; the obese or anorectic may transfer to another form of excess. Attention to the symptom has not solved the individual’s problem of knowledge of the Self. Joining a program that identifies the addict provides a sympathetic environment but does not restore the person to life. Addictive populations have difficulty in relating to the body not because it is distorted but because there is no self-concept to draw on, let alone one that remains constant. In the normal evolution of developmental growth there is a change in the physical body. At certain times the change can be profound. Adolescence not only brings about physical changes in the bodily functions, at the same time there begins a process of physical separation from the family. As the person continues to develop, maturation of the bodily functions occurs. While these physical changes are made visible, it is important for the adolescent, the mature adult, and the elderly to hold the self-concept as the basis of his inner being constant. When the individual has accessed and maintained his core, he will be able to make the transition from his current mirror image, from virtual representation to visualization and finally to symbolization. It is necessary to be able to relate to the picture of himself based both on what he sees and what he knows. The importance of early experiences that define the person as a bodily presence is vital to the ability to grow throughout the various stages of the life cycle. If the child experiences herself as a function of a member of the family rather than as a unique individual who is accepted and welcomed into the family group, stagnating behaviors may be triggered.
154
— Conclusion
A family does have great influence on the growth and development of its members. Parents need to become educators who value each family member in their care. Like it or not, parents are positive and negative role models; children are not necessarily able to sort this out. It is the parents who must be aware of their own behavior about eating and feeding. Excessive talk about dieting or weight by a parent may become a lifelong obsession of the child who is vulnerable to an addictive syndrome. Parents need to be vigilant about early tendencies in their child that identify the addictive process. If such observations are noted and discussed with the family doctor, early intervention may prevent development of an eating disorder or the crossover to another addiction. Children who feel they need to be accepted may start with a drug or alcohol trial to be accepted by peers. Freshman college students are particularly vulnerable to induction into eating disorder behaviors by older students. Bulimic behaviors such as bingeing and purging are popular rituals introduced to the young student. Though college administrators are aware of the presence of eating disorder behaviors on campuses, they have been reluctant to provide remedies either for prevention or intervention. Where it is an issue that has become public knowledge, such as plumbing problems because of the practice of bingeing and purging in the showers, some effort is made to explore the possibility of help for the students. But these have not been addressed as a general policy. Publicity may portray the college in a negative light. The active engagement of the college administration in providing students with a full staff of professional therapeutic counselors to carry on early identification of students at risk for eating disorders would serve to enhance the image of the university. An atmosphere that encourages interaction between the faculty and the students will provide opportunity for discussion of problems before they become entrenched. A trained art therapist on staff would not only be able to serve the student body but offer opportunity as well for the administrative staff and the faculty to air concerns that impact on their ability to educate the young students in their care. Recent events of violence and murder on the campus by student against student is not news. Many of these incidents have happened before.
Conclusion — 155
Violence is often expressed when anger is sustained and repressed. If it can be released and appropriately directed, anger can be contained and violence averted. Art therapy can be used individually as well as in groups. The many expressive avenues are useful for the troubled as well as the healthy individual.
Campaign for Eating Disorder Prevention on Campus A protocol for a college administration to prevent eating disorders was developed at the request of the dean of a women’s college in the Eastern United States: 1. Hotline 2. Monthly weighing in health office, recording of weight 3. Drop-in center 4. Library collection of related articles from professional journals and organizations that serve various addictive populations 5. Revision of cafeteria menu and availability of appropriate foods at times when cafeteria is closed 6. Invitation to staff, students, and parents to attend periodic lectures, films, and presentations on eating disorders (ED) from professionals in the field, both medical and mental health 7. Ongoing expressive therapy group 8. Establish residence crisis team consisting of staff counselor and peer educators 9. Campaign throughout the year to raise consciousness of students to the risks and existence of ED; use of flyers and posters on an ongoing basis—advertising various help available to students 10. Development of exchange with doctor on campus or, if needed, students’ personal physician to identify students who are having problems but are passing 11. Peer educators recruit recovered ED students to serve on team to help identify students at risk 12. Raise consciousness of the connection of ED with other addictive behaviors and through education of professional staff on these issues
156
— Conclusion
The faculty of elementary schools play a key role in shaping a child’s self-perception. Teachers have always been in the role of surrogate parents for the children in their care. Today, they are delegated to serve even more significantly for the children of parents who both work. For these children, because the opportunity for the teacher is manifest, the responsibility of the schools is to staff the school with highly trained and well-motivated individuals. Of course the schools must be a safe and secure environment for both staff and students. Good teaching materials need to be available and free from violence, following a solid curriculum. A well-trained staff that includes professional members: e.g., qualified administrator, nurse, and guidance counselor are usually available. Though training in graduate art therapy programs has been in place since the seventies, with programs intended to produce professionals to serve the schools along with other members of the staff, this goal has not materialized. In New York state training as an art teacher is licensed, but art therapy is legitimized by the American Art Therapy Association, allowing the use of ATR but not providing the needed licensure from the state to qualify for third-party insurance benefits nor admission to the faculty as a member of the guidance team. The addition of an art therapist to the staff of each public school would supplement the work of the guidance counselor or clinical psychologist. The art therapist can aid in early identification of problems in young children and adolescents. Expressive art experiences and intervention, or referral as needed, can prevent the progression of a developing problem. The inclusion of an art therapist would be a valuable asset to any college staff, benefiting students through their emerging maturity. It would be especially useful as a means to keep current about their goals and aspirations. It could also serve to organize their program as they experience some of the intricacies of their studies.
Beyond Discovery: Illumination The ability of the individual to make appropriate connections from body dimension to body image, finally forming a symbol of herself
—
PNBIT: Mirror work with discussion of meaning and connection to tasks involving the senses.
PNBIT: Repetition through different tasks that employ the senses to identify the sign: actualization. Weighing, measuring, seeing, and feeling the body from many aspects.
PNBIT: Art therapy tasks: the process of transformation occurs here. Bringing the unconscious to the conscious.
Awareness of nondiscursive significant form promotes illumination of truth and moves toward symbolic transformation. Expressive virtualization leads to conscious awareness.
Developing child: back and forth—darting and returning for reassurance.
Adolescence: awareness of self as an individual and separate.
Relationship of Stages of Self-Concept to Development
Illusion: true likeness but size is inaccurate and image is reversed. Illusion can become delusion unless it is transformed. In anorexia and obesity distortion becomes entrenched, the patient immobilized.
Infant: dependency on objects
3. Expressive Symbolization Art media
Transitional Stages Toward True Symbolization
2.Virtual Sign Mirror image
Adulthood: able to function on a mature and independent level, to symbolize and use symbol
PNBIT: The combination of phenomenal and nonphenomenal experience in the Body Contour Drawing is a potent act performed by the patient and accesses insight and change.
Patient incorporates memory of physical form and captures constancy of form: that of the self and of others. The ability to transfer from conscious to unconscious modes is made fluid.
4. Symbol Nonphenomenal body image
From Sign to Symbol: The Development of Self-Concept Through Phenomenal and Nonphenomenal Body Image Tasks
Physical: touch, feel, see, mass, hearing, senses are used but access to maturity remains in the unconscious
1. Sign Phenomenal body
Table 6.1
158
— Conclusion
based on truth, lays the groundwork for a positive self-concept. The mirror illusion must be put to the sensory test through virtualization in the Body Contour Drawing and then transformed through the power of creative symbolization to attain belief. Meaning follows from this progression. As Langer (1942) has written, “Meaning has both a logical or rational and a psychological aspect” (p. 53). The patient needs to understand his body both as a primary experience and as an abstract symbol for complex meaning. It is necessary for the patient with a disturbed body image to retrace, actually and symbolically, the history of her self-concept and be allowed to regress in order to repattern her sensory perceptions to retrieve her lost body dimension. The Body Contour Drawing used with other related art therapy tasks in the PNBIT, combined with appropriate medical support, can make an impact on the long-term goal of self-regulation. The method provides the therapist with an armanentarium of rich material that may be integrated into her own course of treatment. When the client compares her own art productions and words over time, she can no longer deny the truth. More compelling than any of the author’s analyses of the case studies are the participants’ own words documenting their illumination and joy in discovering their authentic Self. Real healing and growth begin after the self-concept is made available. That is when the client can decide if this is what she wants for herself. She now recognizes herself as an individual of value for whom she is responsible and deserving of care. Application of the PNBIT is a powerful experience and needs the guidance of a trained therapist. It is not intended as a self-help tool but rather opens new avenues for treatment. This book is about people in pain who are helped to find themselves and activate living. Art therapy certainly helps sick and troubled people to get well. It can also help untroubled people be healthier. More important, it engages the individual to strive toward his highest potential. In so doing we set a new standard for living beyond mediocrity. He has to go through his own fire to alchemize into wholeness. This is the beginning— the real graduation-commencement. Graduation and commencement may seem antithetical; the dilemma is resolved when the solution allows that both are true.
Conclusion — 159
The inclusion of art therapy into all medical, educational, and scientific disciplines will transform the concept of therapy, improve health, activate intellectual and creative capacity, and prevent violence. Scholars, scientists, and artists have tried to explain how art moves the spirit but have never been able to find words that depict its powerful force and numimous quality. Only by experiencing it is it made palpable. The focus on whole brain activity and analysis through the prism of the solar dream is a beginning in the journey toward transcendence. Like the recent acceptance by the National Institutes of Health of alternative medicine, art therapy has proven in practice to be a valuable asset to the medical and scientific communities. For patients who have lived with their problem in denial, the impact of the experience of art therapy is a revelation not only of the problem but of their own possibilities. Art therapy takes a person on a pilgrimage through the dark cave of his despair into an illumination of his spiritual side. It reawakens the creative force and inspires ethical being.
Afterwords: Toward an Ethical Society
Art has always been a part of daily life, everywhere, whether we are aware of it or not. Artists were a normal part of culture in primitive times; when art became a more directed endeavor, artists were considered to be a separate group within a society. Art stemming from shamans, witch doctors, and religious ritual was feared and kept at a distance. Artists will always produce art—no matter the rejection. But left to wander in an inhospitable environment where they are considered to be out of the mainstream, they may become hostile and their work will reflect these feelings. Ultimately, their audience will look upon the artists as cultural guerrillas whose art expresses their anger at their exclusion. Their work may not be popular—but the truth is not against society. It is society. In recent times art therapy techniques have been used to help people to realize health through creative expression. The creative arts therapies, including dance, music and drama, and poetry in addition to visual arts, have been validated as a contribution to the mental health profession. Yet art therapy has still to be acknowledged as a full-fledged member of the professional therapeutic community. Art therapy is tainted by the rejection of art as a vital force in our culture. —
160
—
Afterwords —
161
There is in my opinion evidence that the lack of active art experiences and concomitant saturation with pseudo-art among large segments of the population constitute a pathogenic condition. The art therapist is in a position both to contribute to the understanding of this condition and to help develop methods of dealing with it. (Kramer 1971:5)
When Chairman Sheldon Hackney resigned from the National Endowment for the Humanities, he said, “It was not just the cuts, but I had to spend more time telling the public what we do. I could have spent that on programs.” One of the purposes of government is to create good citizens. The National Endowment for the Humanities is a democratizing force in American culture. The National Endowment for the Arts has the same goal. Jane Alexander, chair of the National Endowment of the Arts, also resigned after a heroic effort to maintain support from Congress. Representative John T. Doolittle of California commented on money spent on unneeded programs. He cited the National Endowment for the Arts: “If ever a Federal agency or program that deserved a trip to the chopping block, it is this sandlot for the cultural elite.” When people who are our political elite charge that cultural elitism is expendable, then we know artists need to be identified and what they do clarified. There is nothing wrong with elitism if that word is understood. Elitism can enhance and help our culture to flourish. The arts have a role to play in reenforcing national values. We need cultural warriors who will go out and incite passions for the use of individual creative force. We have allowed a course of bland and, at times, sterile art. Big and loud is not necessarily strong. An authentic art force, free and responsible, can be a great and positive power. Cultural renegades have to rethink their goals and ultimate transcendence. A culture hospitable to art will be more likely to receive art therapy as a serious profession and provide equal status with other therapeutic disciplines. We are still reading news articles about pictures used in treatment by a variety of health professionals, some untrained in therapeutic methods, without a single mention of art therapy or art therapists. When art is nurtured and valued by our society, when it is respected and even revered, art therapists may then be able to flourish in their own right. Many art therapists are artists, indeed were artists, before becoming art
162
— Afterwords
therapists. A portfolio of quality art is required for admission to many art therapy academic programs. It is important for art therapists to continue to work at their art and allow their art to develop as they grow as individuals. The artist-therapist must become one. Just as one works to increase health in clients, one must also find a way to keep an identity as an artist. He must plant art seeds everywhere. Working to help the well person develop creativity may be an avenue to explore, where art therapy will be honored and its influence widened. (Rabin 93:171–72)
Where there is a lack of art there will be sterile and unfulfilled people. They may yearn for creative activity and repress it. This may cause anger, which may ultimately be discharged in unhealthy ways. Art has the capacity to move the culture to a more ethical society.
Toward an Ethical Society 1. Art experiences are important to the healthy development of all. Creative arts should be an integral part of education, not only in the early school years but in college as well, and continued throughout life. 2. All healthy people have access to their creative energy. 3. People who have access to their creativity are physically and mentally healthy. 4. Physically and mentally healthy people are creatively functioning people. 5. Creatively functioning people are free of inhibiting fears. 6. Creative energy can be released by engendering right educative attitudes in the young and by a process of repatterning the emotions where creative patterns are blocked. 7. A person who thus finds and experiences his individuality will obtain inner freedom. 8. People who experience and are permitted to develop authentic inner freedom (not to be confused with “looseness”) spontaneously develop self-discipline. 9. Self-discipline, the most powerful of all authorities, promotes the climate for the development of a truly ethical human being. 10. Ethical people make ethical societies. 11. An ethical society creates a noble culture.
Afterwords —
163
Relationship to the Self is at once relationship to our fellow man, and no one can be related to the latter until he is related to himself. (Carl Jung, cited in Stevens 1994:125) Self-actualization or health must ultimately be defined as the “Being” of the person. . . . Creativity is . . . a sine qua non of . . . essential humanness. (Maslow 1968:145)
The Art of Art Therapy I am an artist, a printmaker. Creating a woodblock is a lot like therapy. A woodblock begins with a design, drawn on paper, traced in reverse and transferred onto a block of wood. Though there are many different carving tools, I usually use only one to release the image from the wood. Printmaking, in particular woodblocks, is a unique art process. The picture emerges by indirection, that is, you must reverse your image in order to “get it right” and what you carve out will not print—what you leave in will print. The woodblock is called a relief print. So far, the process is a lot like the Mandala task, giving us the safe haven of structure. It is after the design and carving have been correctly transferred to the wood that the most challenging part of the process begins. The printing of the carving offers the artist an infinite number of possibilities. The size and type of paper, the color or colors to be applied, the use of the various burnishers and brayers all contribute to the final work. How about printing the image more than once, upside down, adding the back of the block to the original carving, changing the colors, the transparency, the opaqueness? Even the room and time of year effect how the print will appear on completion. The mood and vigor of the artist on a particular day will effect the strength and mood of the print. Freedom with form: a lot like many life choices. Art, accompanying man on his difficult journey to himself, has always been ahead of him at the goal. (Jung 1931)
APPENDIX 1
Extracts of Exit Tape Recordings
a. Jessica Mason JESSICA:
. . . before the therapy I felt like an elephant—like this enormous
shape with a very timid inside, like a little mouse inside. . . . Now I feel like a small person in shape and very strong inside. . . . Even though I’m big inside, I fit perfectly into this outside body. . . . It’s very nice . . . . THERAPIST: JESSICA:
How does this transfer to your life situation?
I feel solid, strong, and I’m not afraid of everything. Before I was
so scared. . . . I needed constant reassurance that everything was going to be all right. . . . Even if I knew I could, I needed somebody to tell me I could and then I could be mobilized. . . . I just felt scared. Except, I didn’t know what the feeling was. I thought it was unhappiness. . . . I can’t tell you what I was afraid of . . . maybe that I would never be what I wanted to be, or maybe that I wasn’t what I thought I was or that I didn’t recognize myself in the mirror or . . . a combination. I’ve got all the stuff I had before. I know I’m the same person, except now I think I trust myself as being there. . . . Somehow I made myself enormous in my head and what I saw in the mirror was not what I was really seeing. . . . I knew I weighed 183, but what I saw was something grotesque and enormous, like maybe 350 . . . that’s Megan Brown’s recording is included in chapter 5.
—
165
—
166
— Appendixes
how I felt. . . . The more I felt that way, the worse I felt, and the worse I felt the more I ate. . . . I’m trapped in this “I’ll never be thin, I’ll never be able to lose the weight, it’s too much,” and I’d eat and feel terrible because I just made it worse. . . . It was like this circle . . . I was . . . just running around inside myself. . . . It was really fear. . . . Since the day of that contour drawing discovery there hasn’t been a day when I looked at myself and hated myself or felt ugly or bad. . . . I thought I was miserable because I was overweight, but it was so much more. I was in two different places. One, my feelings about myself and my feelings about who I thought I was. But I thought it was just “If I lose 50 pounds, everything will be just fine” . . . I knew from feeling you draw me I had to accept the fact that what I saw was what I was, and no matter what my head said, my eyes told me I was that size and I could not believe that I was so small. It was amazing to lose 150 pounds in a matter of seconds while looking at yourself because I was so small. . . . It was so wonderful to feel acceptable to myself. . . . I’m not this enormous hulking thing. . . . I’m a woman. Even if she’s overweight, that’s acceptable. . . . At that moment it turned it around. . . . It was negative, negative, negative, negative . . . then I hit a wall. All of a sudden everything got shook right and it was positive— OK, OK, OK . . . I just connect . . . I felt like somebody punched me in the stomach. . . . And the feeling went from my stomach to my head, and it was like my eyes were seeing . . . . . . bits and pieces—sort of learning a language. If you taught me three or four phrases in Japanese, I might understand those three or four phrases, but that didn’t mean I could speak Japanese. You could explain to me that I wasn’t 300 pounds, that I was this size, but I didn’t understand. . . . I couldn’t connect it to myself. . . . The weight, my distortion about my weight, and my size was so bad that it was spilling over into other things like my perception of who I was and how I affected people and how they related to me. . . . And it even started to affect how I did things because I felt so bad about myself that I didn’t think I could do anything right. It was like “Look what I did to myself. I’m going to screw up everything.” If you asked me if I was depressed, I would say no. . . . I thought, “I’m functioning fine. I’m just unhappy about the way I look.” That’s what I felt.
Appendixes —
167
I believed it. I didn’t understand until you started helping me pull it back how bad it was. THERAPIST: JESSICA:
What was the worst pain?
. . . Being measured was the hardest thing we did. . . . I didn’t
want to know. . . . If you told me my hips were 50, that didn’t make sense to me. I didn’t understand what 50 was. . . . If it was 50, it was enormous— it was horrible. . . . The connection that I made thinking how I hurt myself over the years, that was the most painful thing I had to deal with . . . that I had inflicted so much pain on myself and I didn’t even know it . . . that was the worst . . . that I needed help and didn’t even know . . . it made me feel saved . . . that sounds so silly . . . I didn’t know I was sick . . . how much longer would it have gone on? It made me angry that I hurt myself in such depth for hardly any reason. . . . I’m not saying that my sister was not important, I’m just saying, “What was the point of all that?” It was so dumb. . . . Now I can look back at it with such clarity. . . . We’re talking about a month ago and about twelve to fifteen years ago. . . . It amazes me that it is so clear to me now. . . . What happened in this room was such a simple thing to cause such an overwhelmingly significant change in my life. . . . I feel I was led— but slowly—up a mountain, but I wasn’t helped up the mountain. Somebody showed me how to climb up and said, “Now you have to follow these footsteps. I can’t pull you.” And I had to walk up this mountain slowly . . . or I would have fallen down, and I got to the top and there was . . . this incredible sunrise or something, and then when the sunrise was done, the same person was down at the bottom, and they said—you said, “OK, now you have to come down slowly and I’ll show you how, but you still have to climb down.” I didn’t expect the sunrise, I didn’t know what was going to be at the top of the mountain. I just trusted you, so I followed you. It was so subtle, and it was so easy, that it never occurred to me that we were going anywhere. And we got there and it was like “WOW! Here we are!” . . . The first going up I had no idea where I was going. . . . Now I know . . . I’m going forward . . . I’m so sure of it. I feel so confident. . . . How can I feel so confident? But I feel capable . . . capable . . .
168
— Appendixes
. . . The nicest thing about this is not acknowledging my size or learning about the distortion or even accepting that. It’s finding out that the person I really wanted to be so desperately and tried to pretend I was I am.
b. Claudia Bernard CL AUDIA:
. . . I’ve learned how to manage my eating. . . . It was a symptom
of other important things that were bothering me . . . It’s not too late. I was beginning to feel overwhelmed by all my problems, and I wasn’t able to accomplish anything [babysitting]. Now I feel I don’t need to do that. I still like children very much. I got it out of my system. I don’t need to do it . . . I have certain goals . . . and I feel that I’m making steps to accomplish them. I understand that I’ve acted in immature ways. . . . It’s way past the time where I should be acting like an adult, a responsible adult. . . . I felt since I was a single person it didn’t really matter what I was doing. I was dabbling here, I was dabbling there, thinking that at some point in my life somebody else will take care of me and it didn’t really matter what I did. It does matter what I do, whether I’m single or get married in the future. . . . I have to take care of myself and the time to do it is now . . . I feel I can do that and I am doing it and I will continue to do it. . . . It’s very important for my own self respect that I do that. Being single, my life didn’t start to begin yet, it wasn’t that important. . . . The times when I grew up, my family, I was treated as being more childlike . . . perhaps I haven’t wanted to be an adult completely . . . that’s the way I will be set for life and I don’t like the feeling of being set into something so permanent that it’s irrevocable. . . . It was wrong for me to isolate myself so completely . . . it only seemed to have served the purpose of depressing me more. I was in a very depressed way and I couldn’t seem to get out of it and yet I knew I needed help. I feel completely different. I feel I’m not depressed . . .I’m not overwhelming myself with tasks. I’m taking one day at a time, doing one thing at a time. I feel I’m accomplishing those goals that I set for myself. I feel I’d like to accomplish some of them a little better, perhaps a little faster, but I’m not being frustrated by it. I’m just continuing with my plan.
Appendixes —
169
(Claudia read directly from a prepared statement into the tape recorder.) . . . I had reached a point where I knew I had to come to terms with myself and I was doing a lot of self-destructive, spiteful things that I realized that I was doing a little on purpose that were disturbing and I decided to cut the crap and help myself, see myself—and this program has done that. I feel for the rest of my life I would like to be working towards selfimprovement and accomplishing the tasks that I set out to accomplish. (Claudia completed reading her prepared statement, then asked to have the tape recorder turned on again. She continues.) By saying the same things and discussing the same things over and over again, it made it sink in better . . . made me realize that there were important things that I had to work on. At first I was annoyed about going over the same questions and the same answers I was basically giving. But . . it was important. Just like looking in the mirror . . . I was forced to look at my body shape, my body image, even when I didn’t want to. And by forcing myself to come to terms with what I actually looked like, forced me to come to terms with other parts of me that I didn’t want to face up to or see . . . I was forced to face up to myself and acknowledge that it wasn’t all right for me to look like this. It made me face reality as far as my weight was concerned and as far as my life was concerned and how and what I wanted to do with my life. I had to face reality. It was difficult. I thought I was being real, but I was ignoring certain important things.
c. Heather Allen THERAPIST: HEATHER:
Six years.
THERAPIST: HEATHER:
How far back does this go?
What was it like doing this?
. . . before [therapy], I looked in the mirror a lot, every ten or
fifteen minutes, to make sure that I was OK, that I was still in control, that I was still thin enough, that my clothes were still falling off. The pattern was—the first thing I would do when I got up in the morning was try something on to see if I had lost weight overnight, to see if I was thinner than I was when I’d gone to bed. . . . It was always just a measurement
170
— Appendixes
of were my bones sticking out. . . . If I felt insecure or intimidated or frustrated at work, if something were not working out, I would go into the bathroom and see how thin I was all the time. . . . It made me feel good, it pumped me up. THERAPIST: HEATHER:
Has it changed at all now?
Now I understand intellectually and rationally that I have to
eat for nourishment, period, three times a day. I want to relieve the anxiety that goes along with starving yourself for a day. I love to do it, but it was frustrating to see other people eat and me not to be able to. . . . I created a lot of anxiety in dealing with other people socially. . . . They would get mad at me if I wouldn’t eat or . . . if I did eat, and then I would worry about it and complain, then it was a constant problem for them, too. So, knowing that I’m going to be able to eat in a couple of hours is a great relief. . . . It just took a long time to do that. And you’re not going off the deep end. The scale’s not going to go berserk. . . . I can enjoy things a lot more because everything doesn’t revolve around food as much. It’s not completely gone, but I can just enjoy life a lot more. . . . Even though my weight’s not what I want it to be . . . it’s still scary. But . . . I just understand that I’m still underweight at 125. I’m 5 feet 9 inches . . . the minimum should be 130–135. . . . I mean, even 140 wouldn’t be outrageous. THERAPIST: HEATHER:
What has happened?
In the last seven months I’ve gotten a grip on eating. I’m not
panicking . . . it doesn’t take over. . . . I’m a little more in control of the food, which is sort of translating the control, I guess, taking it off of me and putting it on the food. Before, if it was there, I would eat everything, it was a big monster. THERAPIST: HEATHER:
What about getting up at night [to eat]?
That’s going away . . . probably by eating enough food all day
[now] . . . I wasn’t hungry at two o’clock in the morning. THERAPIST: HEATHER:
How else did it change?
Understanding that the mirror is not reality, that it is distorted,
and understanding that my perception is distorted, I didn’t realize that
Appendixes —
171
for the longest time, but my perception is distorted. . . . When I would draw things from memory and I would trace over them, they were usually twice the size of what was real. . . . I probably do that when I look in the mirror and I probably eliminate myself and just expand it visually. I have a perception problem. From looking in the mirror and stepping on the scale every week and having a record of it I realize my perception [is off]. THERAPIST: HEATHER:
How has this affected your functioning?
The agoraphobia has gone away. . . . I was afraid I was going
to eat too much if I stayed home, I would eat everything in the refrigerator. Then I was afraid to go outside, I was afraid something was going to happen to me . . . then I was afraid to go out at lunch, to go out of the building. It was so irrational . . . I was afraid to be alone, but more afraid to go outside. It’s not a problem at all anymore. It feels real good to be in control of my own decisions and not relying on him [boyfriend] for my happiness, to cook my food, or take me out to dinner and make sure I eat . . . and not dumping on my friends, and making sure I eat or don’t eat too much. It’s not their problem, it’s my problem. I can deal with it. . . . You said, “The food is not jumping into your mouth.” I had never thought about that before. I had never thought about the fact that I was going to be able to eat in another three or four hours. It’s a whole new concept. I found myself reacting to people differently at work. I came to the realization that I don’t have to explain myself all the time. I don’t have to make excuses or talk. I understand and realize I have to weigh a little bit more. That’s going to mean having larger breasts and having hips and even though I don’t like the way it feels, I’ll probably get used to it, and that’s the way it is. I’m much calmer. People that don’t even know anything, tell me I seem awfully at peace, calmer, that I look healthier. People tell me I look better than I have in my whole life. . . . Before I started dealing with it, everything was a gray haze. I couldn’t really see anything—things in nature—going for walks, everything was hazy and gray to me because I was consciously aware of my stomach and how much I weighed [so] that I couldn’t think about anything else. I didn’t enjoy doing anything else. I didn’t enjoy just sitting and talking with
172
— Appendixes
someone because I was constantly sucking in my stomach. I couldn’t do anything. . . . Everything had a cloud on it. Everything was sort of through a gray mist. I couldn’t really focus on anything—would be lethargic. Now it’s so wonderful to go eat lunch and function in the afternoon. It’s like—fun! It’s amazing! Or to eat breakfast and go to work, and not feel horrible and to look forward to the meals. I really look forward to . . . the meals! I really look forward to waking up in the morning. Even if I feel I’ve eaten too much, still it doesn’t matter. . . . It’s not the end of the world. I can go on and do other things—that’s the most fun of all.
d. Linda Miller LINDA:
(Discussing knitting a sweater for herself ): I liked the pattern and
picked a small size and measured the gauge to make sure the sweater would fit me. . . . After it got all finished . . . it’s too big in back and it hangs like most jackets and other clothes that I try to buy in the store, I did not wish that I were the size to fit it. I wished that the sweater was right for me. Using the knitting gauge, I measured it. Evidently I’m smaller than the pattern calls for . . . than the standard small pattern. (Discussing the Body Contour Drawing): I was astonished the day you drew me up on the wall. I couldn’t believe it was me up there. The person was too small. It looked very small. Especially the hips. It was different the times I’ve looked in the mirror and seen me in the mirror and thought something was wrong with the mirror. [The contour drawing] . . . was actually me. It was drawn to my contour and I believed it. I saw you do it. You didn’t cheat. . . . If you had done it the first time I would have thought you were making fun of me . . . (Discussing the concept of being in “control”): Work situations are sometimes beyond your control. If I had been a man I might have had a different profession or gotten farther or been somewhere else. . . . When I got started in the business world, it was different. I’m at that age, over fortyfive, nobody stands a chance—being primed for the top, man or woman. I feel . . . things should have been different. . . . Now there’s no way, it’s too late. (Linda discusses the concept of “going out of control”): If you’re driving a car and you’re going to a certain place and you lose control, you’ll never
Appendixes —
173
get there. You might have an accident. You’ll crack up. . . . I had a girlfriend who a couple of times tried to commit suicide. . . . I never really felt that way, I never really thought about it. It’s a very distasteful thought to me—although once in a while—I have been driving a car and being very depressed and saying, “I could let go of the steering wheel and that would be it, because you know, driving at 60 miles an hour . . . when the moon is full . . . it could be any number of things . . . last winter . . . work wasn’t going right. . . . I sometimes feel I’m much too alone . . . (She lapses into a discussion of an evening she had planned with her boyfriend ): He was going to stay over—and he came in with this terrible, terrible migraine headache. He was feeling sick, nauseous. He stayed over for awhile and then he decided he better go home because if he was going to be sick, he wasn’t going to inflict it on me. So he’ll just go home and stay there in case he didn’t feel like getting up in the morning. After he left I evidently was upset, angry, I don’t know why I should be angry if he’s got a migraine headache. Seems to be beyond his control and I went into the kitchen and ate for awhile and I knew why I was doing it. . . . I could have insisted that he stay anyway. I don’t know if that would work. After that I don’t know . . . sometimes you almost analyze people you know, you think they’re going to do something or make a certain move and they don’t do it and really shocks you. You make an assumption and you’re wrong. . . . I never go to singles functions. Most of those things are chock-full of women . . . and there’s all that competition. (After this, Linda talked about her relationship with John as a reflection of her need for a father figure. . . . Linda then discusses hunger, satiation, appetite, eating.) THERAPIST:
LINDA:
What is food hunger?
I never really experienced what you would call hunger pains. When
I get hungry and haven’t eaten for a long time, I get cranky and teary. But I don’t have any physical feeling—pains in my stomach. I really don’t know what hunger is. I may be hungry [but] physically, I don’t feel it. [Food hunger is] physiologically necessity for food. Myself, I don’t have any triggering mechanisms. THERAPIST:
Describe your food hunger.
174
— Appendixes
LINDA:
My food hunger is personally more psychological. I think I want
something or need something. If blueberries are in season, I would develop a craving for blueberries. THERAPIST: LINDA:
Appetite is the ability to eat or consume food.
THERAPIST: LINDA:
What is appetite?
What is your feeling of satiation?
The feeling that the food is up to here, the feeling of overstuffing.
More than just being satisfied. THERAPIST: LINDA:
Where is hunger for you in your body?
Hunger should be in the stomach. It is mostly in my mind. I don’t
ever remember being hungry. My mother said I was very normal as an infant and child. I ate good and I never fussed. I was very thin and then got very heavy. I didn’t think about food. . . . A few times when I hadn’t eaten all day and just started to cry or started to get very cranky, or on a rare occasion, I remember . . . I had breakfast, didn’t have time to have lunch. I was shopping with a boyfriend. I said, “I don’t want to go into any more stores!” I was just in tears, I was hungry. As soon as he fed me, I was fine. . . . It happened once later on. I obviously get crazy when I’m hungry. Whiney, like a child. THERAPIST: LINDA:
During eating I try to savor every morsel.
THERAPIST: LINDA:
What do you feel during eating?
After eating?
After eating I don’t want to stop. I get these feelings . . . Sometimes
I go all day [without eating], but once I start . . . all I think about [is the food]. Afterwards, I wonder why I ate so fast and I keep thinking about food. . . . I don’t ever really get satisfied. That’s the problem—always this need to have more. I eat food until I go to bed . . . THERAPIST: LINDA:
What could satisfy you?
Probably companionship—love and affection. Shows that I’m not
getting it now. At home I’m one of those closet people . . .
Appendixes —
175
When I feel I’m overeating, I now try to ascertain if I am angry . . . and if so, why, or at whom . . . father, mother, myself. If I’m angry at myself it’s because I feel I should be accomplishing something, reading, writing, weaving, etc., instead of eating. Sometimes I think I eat because I’m bored and don’t seem to find anything to “turn me on” or get enthusiastic about. In previous years when I’ve gotten interested in something . . . I could work all night with no thought of food. (Here, Linda discusses her reaction to participating in the study): I’m not as unhappy as I used to be when I started to come here. But I wonder why I get the feeling of elation of being down at the bottom of the pendulum. Reason: “Oh, good. My weight is down. Now I can go out and eat more.” That’s not normal or the way I should feel. A reward. When my weight goes up now I don’t panic as much. I don’t necessarily say, “OK, I won’t eat today.” My relationship with my mother is much improved, i.e., more open. Much to our surprise, she seems quite happy about the growing relationship between my sister and myself—I was amazed at how my drawings reflected my feelings or observations—much better than I could express them (or was willing to!). I still think about food often, try to plan my day around not eating, then eat continuously when I go home. Still feel compulsive, need to swim or exercise every day—get grumpy when I don’t do anything. More aware of what I should do or shouldn’t do, just have trouble doing it. Still like to see the scale at 102 but don’t feel as panicky as I used to when it goes to 105, 106. I have found this whole experience amazing. . . . It’s fascinating and it’s almost unbelievable that this can happen in this way . . . THERAPIST: LINDA:
Talk about the drawings and things that surprised you.
The one with my boss and me on the outside of the Mandala—I
don’t think it could have been expressed any better in words. The family portrait and the way it changed was fascinating. But also I never thought of things in those terms. I certainly had to think a lot more about what I’d like to do, what I’d like to be, what I’m trying to do. THERAPIST:
In what areas?
176
— Appendixes
LINDA:
Why I’m having problems. What I’ve been thinking about. Why
am I living this existence, not allowing myself to have, in effect, a total life, and just pieces of a life? Why have I been reticent to not be more pushy at work, more affirmative, not so aggressive . . . to get myself to do things the right way there, so that I would be farther ahead? . . . At the same time, I know I have these feelings about “Well, if I do get farther ahead, then I’ve got more responsibility and do I really want that?” and I have still not been able to get that balance within myself. THERAPIST:
LINDA:
Has this transferred to your life in anyway?
The fact that we (my sister) went to the cemetery and I told her
about (John) made her relate to me more than she had in the past. I don’t know how she thought of me other than being mother’s girl because there were always sides in the family, and [I’m] probably not very normal, [I’m a] very strange person, because I never talked about men in my life and never talked about doing other things or even going out with the girls much. I just didn’t have many friends. And it [the project] . . . helped with my mother. At first I thought she’d be upset about my telling our life history to some strange person. She seemed to feel that would be good for me because she’s worried that she has poisoned me . . . against men. That’s her biggest fear, that the whole situation at home . . . If I go through something like this and can help myself with my supposed eating problem . . . I say “supposed” because nobody believes I have an eating problem. They look at me and say, “you’re thin! How can you have an eating problem!” THERAPIST:
LINDA:
Discuss that a little bit.
I feel it’s an eating problem because I’m always thinking about
food. I eat late at night when I’m not hungry anymore. If I’m not eating, I’m chewing or I’m sucking on candy. There’s always something in my mouth . . . I’m even doing a self-destructive act that way because my teeth are not that good and I know I should not be doing it for my teeth as much as for my figure or my body. THERAPIST:
What do you weigh now?
Appendixes —
LINDA:
177
I weigh 104½ today, and it sounds insane—that’s why I say a “sup-
posed eating problem,” but I feel it’s a problem because I’m always thinking about food. The perception is different. It’s a little crazy to worry about my weight when I’m this weight. But the constant obsession with food is probably what’s more of a problem than the actual gaining or losing of a couple of pounds. It sometimes interferes with what I want to do because “I gotta go eat.” Therefore I can’t weave or therefore I can’t read this book or therefore I can’t do this. I got to have something to eat. THERAPIST: LINDA:
Has this changed in any way?
I’ve been trying harder to eat regularly, regular hours, which I
didn’t do before. . . . I’m not always succeeding. I still tend to have no willpower. When food is around, there’s candy out at work, I have to grab a piece as I walk by. I can’t leave it alone. I’m not so much a cake eater, so cake I can leave alone. THERAPIST: LINDA:
Any thoughts about what may be causing this?
Well, obviously some of it is due to anger and the pushing down
of anger because I don’t express it very well or at all. But there are some times when I’m eating late at night and I’m not hungry and I’ve had plenty to eat and I really can’t figure out if I am hungry at that point who I’m angry at or who the anger is toward, maybe toward myself and I don’t realize it. I can’t imagine that it can only be anger, though. There must be some other emotions that I’m repressing that may also be causing this. THERAPIST: LINDA:
What do you think they might be?
Loneliness . . . could be unhappiness with myself but that could
be anger . . . or for not doing something or not getting somewhere or not accomplishing something. The more I do it the worse it gets. . . . If I say “Stop eating, go and do some weaving” and I don’t do the weaving, then I get angrier and angrier and keep eating—so nothing gets done. . . . It takes awhile to sink in . . . to explore your own self. Now I imagine that five years from now when I’m way far away from this, that it’s still going to stay with me and that at any times of crisis or problems it will be useful then. That’s the way I feel about it right now . . .
178
— Appendixes
THERAPIST: LINDA:
What have you discovered?
I discovered that deep down inside I am a very angry person. I
never realized that. I always considered myself calm, cool, and collected and just rolled with the punches and took everything as it came and it really didn’t disturb me, but obviously it has. THERAPIST: LINDA:
What else?
I probably have not as good a self-image as I should and . . . I
haven’t figured out why. That’s still a problem. I discovered that if I gain 3 pounds, nothing happens—really, other than my belt gets a little tight. . . . The sessions were a lot of work. Sometimes I would leave here quite tired, but . . . I never felt like not coming, never been negative . . . long sessions have come out of interest and subjects that matter. . . . I’m trying to look in the mirror and talk to myself and try to make it change . . . in seven months we’ve made a lot of progress. I would like not to do this [eating problem] anymore. It will take a long time, but I’ve made a start. I’m trying to express myself more and I’m trying to eat more normally and more regularly. I’m talking to myself a lot more when I am not doing what I’m thinking I’m trying to do. I’m analyzing myself. Unfortunately, it allows me to still eat and analyze at the same time, but I think that’s good. . . . I say, “Oh well, you did it last night, maybe you can not eat so much today.” But it doesn’t seem to color my whole attitude for the day, which it did before. I would be totally a nonperson and irritable. THERAPIST: LINDA:
What was the major thing that was useful?
I know I felt better about my relationship with my sister. One of
the useful things I drew was the picture I drew sitting at the TV in a third direction. . . . In the clay, I left my mother out. I keep putting my father in the family and left my mother out. [Mandalas]: I was more protected inside. [Body Contour Drawing]: I didn’t realize how small I was. [Weighing and measuring]: Is good for me because I tend to think I’m overweight so I will not get on the scale. So, by having to get on the scale once a week [it] puts me back in perspective. Where some days I come and I say, “Oh my God, she is going to weigh me,” and I imagine I weigh 120 pounds and I only weigh 104, and I say, “It’s not so bad.”
APPENDIX 2
Self Report
—
179
—
TASK
SELF ANALYSIS
MIRROR VIEWING
WEIGHT
COMMENTS
SANDWORLDS
HTPPA
MANDALA
SELF BOX TITLE
CONTOUR DRAWING
KFCS
COMMENTS
CFLD
BDEM
7. OUTER APPEARANCE
6. INNER FEELING
5. EYES
4. SKIN
3. MAKEUP
2. HAIR
1. FACE
Home
Office
LBS.
Address ___________________________________
Accepting
Rejecting
No opinion
Telephone _________________________________
Name ___________________________ Age ______
Date ___________________
PNBIT SELF REPORT
Session No. ______________
180 — Appendixes
APPENDIX 3
Therapist Report
—
181
—
SPECIAL NOTES
HEALTH PROB.
Relationship to Investigator
COMMUNICATION
AFFECT
TASK
SELF ANALYSIS
Office
MIRROR VIEWING
Depressed
Verbal
SELF BOX
SANDWORLDS
CFLD
MANDALA
HTPPA
BDEM
Home
LBS
WEIGHT
TSCS Stable
CONTOUR DRAWING
KFCS
Address ___________________________________
Color Notes:
Title:
Nonverbal
Agitated
Telephone _________________________________
Name ___________________________ Age ______
Date ___________________
PNBIT THERAPIST REPORT
Session No. ______________
182 — Appendixes
APPENDIX 4
Sequence and Time Chart
—
183
—
DATE
TSCS
CFLD
HT/P
SES: Session # TSCS: Tennessee Self Concept Scale CFLD: Chromatic Family Line Drawing HTP/P: House/Tree/Person/Person/ Animal (Pencil) HTP/C: House/Tree/Person/Person/ Animal (Chromatic)
SES 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24
NAME
HT/C
SB
SW
ADDRESS KFCS
BDEM
BCD
M: Mandala SB: Self Box SW: Sandworlds KFCS: Kinetic Family Clay Sculpture BDEM: Body Dimension Estimate and Measurement BCD: Body Contour Drawing
M
SD
MV
BIRTHDATE EQ
HGT
WGT
SD: Spontaneous Drawing IC: Informed Consent EQ: Eating Questionnaire/History MV: Mirror Viewing HGT: Height WGT: Weight PRF: Physician Release Form
IC
PRF
184 — Appendixes
APPENDIX 5
Outline Drawings: Figure Selection, Male
I
A
H
B
C
G
D
F E Name ______________________ Date _______________________
Please circle letter of figure which most closely resembles your own at this time. A = Thinnest
I = Fattest
—
185
—
APPENDIX 6
Outline Drawings: Figure Selection, Female
I
A
H
B
C
G
D
F E Name ______________________ Date _______________________
Please circle letter of figure which most closely resembles your own at this time. A = Thinnest
—
186
—
I = Fattest
APPENDIX 7
Body Dimension Estimate and Measurements: Linear, Male
—
187
—
188
— Appendixes
M ALE E: _____ Head M: _____ Width at Temple
Head Length E: _____ M: _____
E: _____ Neck M: _____
Shoulder E: _____ M: _____ Upper Arm, Shoulder to elbow E: _____ M: _____
Torso, Shoulder to Buttocks E: _____ M: _____
Lower Arm, Elbow to wrist E: _____ M: _____ Hand E: _____ M: _____
Upper Leg, Hip to Knee E: _____ M: _____
Lower Leg, Knee to Sole of Foot E: _____ M: _____
Foot, Heel to Toe E: _____ M: _____ Name ___________________ Date ____________________
LENGTH
APPENDIX 8
Body Dimension Estimate and Measurement: Circumference, Male
—
189
—
190
— Appendixes
M ALE Head above Ears E: _____ M: _____
Neck E: _____ M: _____
Chest E: _____ M: _____
Upper Arm E: _____ M: _____
Waist E: _____ M: _____
Elbow E: _____ M: _____
Hip E: _____ M: _____
Wrist E: _____ M: _____
Upper Thigh E: _____ M: _____
Knee E: _____ M: _____ Calf E: _____ M: _____
Instep E: _____ M: _____
Ankle E: _____ M: _____ CIRCUMFERENCE Name ___________________ Date ____________________
APPENDIX 9
Body Dimension Estimate and Measurement: Linear, Female
—
191
—
192
— Appendixes
FEM ALE E: _____ Head M: _____ Width at Temple
Head Length E: _____ M: _____
E: _____ M: _____Neck
Shoulder E: _____ M: _____
Torso, Shoulder to Buttocks E: _____ M: _____
Upper Arm, Shoulder to elbow E: _____ M: _____ Lower Arm, Elbow to wrist E: _____ M: _____ Hand E: _____ M: _____
Upper Leg, Hip to Knee E: _____ M: _____
Lower Leg, Knee to Sole of Foot E: _____ M: _____ Foot, Heel to Toe E: _____ M: _____ LENGTH Name ___________________ Date ____________________
A P P E N D I X 10
Body Dimension Estimate and Measurement: Circumference, Female
—
193
—
194
— Appendixes FEM ALE Head above Ears E: _____ M: _____ Neck E: _____ M: _____ Breast E: _____ M: _____
Upper Arm E: _____ M: _____
Waist E: _____ M: _____ Hip E: _____ M: _____
Elbow E: _____ M: _____ Wrist E: _____ M: _____
Upper Thigh E: _____ M: _____ Knee E: _____ M: _____ Calf E: _____ M: _____ Ankle E: _____ M: _____
Instep E: _____ M: _____ CIRCUMFERENCE
Name ___________________ Date ____________________
A P P E N D I X 11
Sandworlds Grid
1
2
3
4
5
6
7
8
A
A
B
B
C
C
D
D
E
E 1
2
3
4
5
6
7
8
—
195
—
A P P E N D I X 12
Questionnaires
a. Eating Questionnaire Name _________________________________
Date ____________________
Date of Birth ____________________ INSTRUCTIONS: Please answer each question. Back of form may be used if
necessary. Please identify answers on back of form by question number.
1. What is your eating problem? 2. a. Do you consider yourself to be a fat person?
Yes ___
No ___
Yes ___
No ___
Yes ___
No ___
Yes ___
No ___
Yes ___
No ___
b. Why? / Why not? 3. a. Do you consider yourself to be a thin person? b. Why? / Why not? 4. a. Do you like being fat? b. Discuss this. 5. a. Do you like being thin? b. Discuss this. 6. a. Do you know how much you really weigh now? Give weight ______
—
b. Do you consider this to be fat?
Yes ___
No ___
c. Do you consider this to be thin?
Yes ___
No ___
196
—
Appendixes —
d. Do you consider your current weight to be a good weight for you?
197
Yes ___
No ___
Yes ___
No ___
Yes ___
No ___
Yes ___
No ___
Yes ___
No ___
Yes ___
No ___
Yes ___
No ___
Yes ___
No ___
e. What is your ideal weight? ______ lbs. f. How much should you weigh? ______ lbs. g. How much would you like to weigh? ______ lbs. What is your height? ______ ft. 7. a. Have you ever been thin? b. Give weight _____ lbs. age _____ yrs. Year _____ c. Did you like being thin? d. Discuss this. 8. a. Have you ever been fat? b. Give weight _____ lbs. age _____ yrs. Year _____ c. Did you like being fat? d. Discuss this 9. a. Did any important event happen during your fat period? b. Describe and discuss 10. a. Did any important event happen during your thin period? b. Describe and discuss 11. a. Has anyone ever called you “fat” (or similar) to your face?
b. What name did they call you? ________________________________ c. How old were you? ______ yrs. d. Discuss the circumstances e. What were your feelings? f. What action did you take? 12. a. Has anyone ever called you “skinny” (or similar) to your face?
Yes ___
No ___
b. What name did they call you? ________________________________ c. How old were you? ______ yrs. d. Discuss the circumstances e. What were your feelings? f. What action did you take? 13. a. Have you ever had a good experience because of being fat?
Yes ___
No ___
b. Discuss this. 14. What is the worst experience you have had related to being fat?
198
— Appendixes
15. a. Have you ever lost out on something because of being fat?
Yes ___
No ___
Yes ___
No ___
b. Discuss this. 16. a. Have you ever had a good experience because of being thin? b. Discuss this. 17. What is the worst experience you have had related to being thin? 18. a. Have you ever lost out on something because of being thin?
Yes ___
No ___
Yes ___
No ___
Yes ___
No ___
b. Discuss this. 19. a. Do you ever envision yourself fat? b. How fat? Give weight ______ lbs. c. What is your reaction to this idea? 20. a. Do you ever envision yourself thin? b. How thin? Give weight ______ lbs. c. What is your reaction to this idea? 21. a. Whom do you admire who is thin? ____________________________ b. Why? 22. a. Whom do you admire who is fat? _____________________________ b. Why? 23. How much would you like to weigh? ______ lbs. 24. What size clothing would you like to be able to wear? 25. a. Do you consider yourself to be attractive?
Yes ___
No ___
Yes ___
No ___
Yes ___
No ___
b. In what way? 26. a. Do other people consider you to be attractive? b. Why? c. Do you believe they are sincere? d. Why? 27. What is your best asset? 28. a. Whom do you blame for being fat? ____________________________ b. Why? 29. a. Whom do you blame for being thin? __________________________ b. Why? 30. What do you believe to be the cause of your eating problem?
Appendixes —
31. a. Are you proud of your achievements?
Yes ___
199
No ___
b. Which ones? _______________________________________________ c. Why? 32. What goal in your life would you like to achieve? 33. a. Do you have high self-esteem?
Yes ___
No ___
Yes ___
No ___
b. Why? / Why not? c. Has this been different at other times in your life? d. Discuss this. 34. What meaning does wieight have for you? 35. How do you think being fat has influenced your life? 36. What is the worst thing about being fat? 37. What’s good about being fat? 38. How do you think being thin has influenced your life? 39. What is the best thing about being thin? 40. What is the hardest thing about being thin? 41. Do you believe you are an easy-going person?
Yes ___
No ___
42. Do you always feel easy-going?
Yes ___
No ___
43. a. Do you consider yourself to be a sensitive person?
Yes ___
No ___
Yes ___
No ___
Yes ___
No ___
b. In what way? c. Are you sensitive to others? d. In what way? e. Are you sensitive to yourself? f. In what way? 44. a. What is your job? ___________________________________________ b. Do you enjoy your job?
Yes ___
No ___
c. Do you feel your efforts are appreciated?
Yes ___
No ___
d. How does that make you feel? 45. If you could change one thing in your life, how would you? 46. a. Do you consider yourself a proud person?
Yes ___
No ___
Yes ___
No ___
b. In what way? 47. a. Do other people tend ot push you around?
b. Who? _____________________________________________________ c. How?
200
— Appendixes
48. a. Do you participate in a physical sport, activity, or exercise of any kind?
Yes ___
No ___
b. Describe activity ___________________________________________ c. How often and for what length of time? ________________________ d. Are you an active person?
Yes ___
No ___
b. Body Contour Drawing (BCD) Questionnaire Name ___________________________ Weight ______ Date ______________ NOTE: This questionnaire is to be used in a verbal exchange with the client,
after completion of the first Body Contour Drawing. This questionnaire is repeated after completion of the second Body Contour Drawing. The answers to each question are to be written down by the therapist and used to compare the first BCD with the second.
1. How old is that person? 2. Is that person in good condition? 3. What is that person doing there? 4. What is that person thinking? 5. What is that person feeling? 6. Where is that person? 7. What is that person’s personality? 8. How much does that person weigh there? 9. Is this different from reality? How? 10. Where is that person going? 11. Where is this person coming from? 12. What’s good about that person? 13. What does this person need? 14. Will the person get it? 15. What problem does this person have? 16. What’s the best thing about this person? 17. What’s the worst thing about this person? 18. Where is that person now? 19. If you could change one thing about this person, what might it be? 20. Who is that person? 21. Is that someone you know? Discuss. 22. Do you care about that person? Why? How? Why not? 23. Do like that person?
Appendixes —
201
24. Say one thing about that person. 25. Who is that person? Say name. Say me.
c1. Self Box Questionnaire Name _________________ Date ________________ Self Box # ___________ Use for Self Box 1 and Self Box 2
1. Why did you choose this box? 2. What does the shape of the box suggest? 3. Did you have a plan for the box when you were looking through the magazines for images? 4. On the outside, which is the most significant picture? Why? 5. Which inside picture is the most significant? Why? 6. What are the differences between the inside and the outside? 7. Is there a connection between the inside images and the outside images? How are they connected? 8. What do the outside pictures portray as a whole? How? 9. What do the inside pictures say as a whole? How? 10. Is there a theme which runs through the images? Discuss this. 11. What might a title be for your self box? Sign, date, and title box. 12. What do you learn about yourself from this exercise? 13. What do you confirm about yourself? 14. What changes would you like to make? 15. Do you have any observations about the box? The manner in which it was executed, does it relate to your way of doing a task?
c2. Comparison of Self Box 1 and Self Box 2 Name _________________________________ Date _____________________ 1. Why did you choose box 2. Is this different from box 1? How? 2. Was your approach to doing Self Box 2 the same or different from Self Box 1? Was it more structured or less, i.e., looking for the pictures? 3. Do the inside pictures of 2 and 1 differ in theme? How? How are they similar? 4. Do the outside pictures of 2 and 1 portray similar or different themes? How do they remain the same? 5. Is the significant picture on the outside of 2 different or the same as 1? Discuss this.
202
— Appendixes
6. Is the significant picture on the inside of 2 different or the same as 1? Discuss this. 7. What are the differences and similarities between the main themes in 2 and 1? Images, colors, size, feeling tone? Is there a general difference? 8. What do you learn about yourself from comparing the two boxes? 9. What do you confirm about yourself from comparing the two self boxes?
A P P E N D I X 13
Medical Release Form
Release of Information Re: ____________________________ I hereby authorize Mury Rabin to receive from (physician) _______________________________________________ _______________________________________________ _______________________________________________ information on myself specifically related to eating problem. The purpose of this disclosure is medical information relating to eating problem: diagnosis, treatment, and outcome. Signed ________________________ Witness _______________________ Date __________________________
—
203
—
A P P E N D I X 14
Medical Questionnaire
Date of First Visit ____________
Patient’s Name _________________
Date of Last Visit _____________
Birthdate ______________________
Is Patient in Treatment Now? ______
Doctor’s Name __________________
1. Please describe the above-named patient’s weight problem: _____________________________________________________________ 2. What treatment(s) did you prescribe? Please be specific. Medical __________________
Exercise _______________________
Nutritional _______________
Behavioral _____________________
Dietary ___________________
Psychological ___________________
Medication _______________
Other _________________________
3. What was the response of patient toward treatment? 4. What was the outcome of treatment? 5. Please indicate other medical problems of the patient. Diabetes _________________
Metabolic imbalance ____________
Heart Disease _____________
Surgical _______________________
Amenorrhea ______________
Arthritis _______________________
Endocrine imbalance _______
Other _________________________
6. Indicate your impression of patient in relation to her eating disorder. (Use back of form for further comments) Do you wish to receive a copy of this study?
Yes ___
No ___
Physician’s Siganture _____________________________ Date ____________ Address _________________________________________________________ —
204
—
A P P E N D I X 15
Abstract from “The Yo-Yo in Art Therapy: The Use of Art Therapy in Eating Disorders”
This work represented the use of art therapy as a group experience with obese women, known as “yo-yos”: obese individuals who had successfully lost weight in diet control groups and then regained it one or more times. A variety of familiar art media was used: paint, crayons, clay, collage, etc., incorporating special art therapy exercises, such as the group picture, the group mural, and the “self box.” Tasks relating to body image were assigned; mandalas were used throughout. The art work produced was used as a starting point for group discussions to effect better understanding of the psycho-dynamics of obesity; The scope of the study was an exploratory first-phase observational data collection that involved, at various times, twelve women who were seen over a period of fourteen months, from July 1976 through August 1977. A comparison of two female drawings made one year apart by the same individual suggests a change in body image concept had occurred during the course of the study. A questionnaire administered to this individual at the outset of the study and then again, one year later, appears to confirm what is in the drawings: that alteration in self-view had taken place. Rabin suggests that art therapy offers promise in helping obese patients to put into proper balance distortions in body image and to experience expressive communication
—
205
—
— Appendixes
206
through nonverbal means as a route to control of destructive eating patterns. Rabin quotes Dr. Hilde Bruch in her book, Eating Disorders: “Patients who suffer from anorexia nervosa cannot be cured without a change in body image concept.” Rabin suggests that the use of art therapy for both syndromes might offer a new approach to treatment, especially if focused on tasks involving body image. Rabin applied some of the tasks used in “The Yo-Yo in Art Therapy” in a program in the obesity clinic at St. John’s Hospital in Yonkers, New York. This data collection was used as a starting point for the research protocol in “Phenomenal and Nonphenomenal Body Image Tasks in the Treatment of Eating Disorders” (Rabin 1987). The final form included work with other addictive behaviors, including alcoholism and illegal drug abuse as well as early sexual abuse.
A P P E N D I X 16
Art Therapy Images as an Index to Suicide
Where there are feelings of anger, a sense of harmfulness to others, guilt— that others, or a particular person will be better off without the patientself hatred, hopelessness-drawings can be helpful to identify thoughts or plans for suicide. The pictures can be useful not only to the treating professionals but to the patient as well. It allows the person to see, perhaps for the first time, the extent of his despair. The expressive work allows a third element, an opportunity to distance the patient from the therapist. This sets a more neutral atmosphere in place where ventilation, release and catharsis can occur. It enables communication to begin, providing continuing contact and defining the therapeutic work ahead. While art can be quite specific, it is often ambiguous and abstract. One symbol that has been observed in many patients’ art is the spiral (Wadeson 1980). It can take the form of a whirlpool, turmoil, usually starting out as a broad spiral and progressively becoming narrower. It can be seen as a narrowing range of possibilities, a feeling of being entrapped, with pervasive anxiety and hopelessness as features. While art therapy shows the patient and the viewer where he is at a particular time in his life, some drawings tap deeper into the unconscious, producing thoughts and ideas which have not yet become conscious. It can, in a sense, be an index to future behavior. —
207
—
208
— Appendixes
This can be of value in planning intervention strategies. One method that uses the picture as a means to change the outcome, asks the patient to change the picture, “make it a better outcome,” by having the patient copy his original drawing on another piece of paper and altering some features making it more positive. Discussion of how the patient could actively participate in making this come about gives him a feeling of power over events. Any suspicion that the patient is contemplating violence to himself or others must always be taken seriously, even if this has been observed previously. I have had the experience of seeing violence in the drawing of a patient; his clinical psychologist was deceived by the patient’s verbal exchanges. One look at the drawing told the story: violence against the client’s mother was on his mind. Intervention prevented what might have been an act of rage. Where there is an issue of suicide, or other violence, ongoing care and contact should be maintained. Assessment, an evaluation for supervision in hospital, can be integrated with ongoing treatment.
A P P E N D I X 17
Metropolitan Life Insurance Height and Weight Tables and Frame Size Estimate Chart (1983)
1983 Metropolitan Height and Weight Tables Men Height Feet Inches
Women
Small Frame
Medium Frame
Large Frame
Height Feet Inches
Small Frame
Medium Frame
Large Frame
5
2
128–134
131–141
138–150
4
10
102–111
109–121
118–131
5
3
130–136
133–143
140–153
4
11
103–113
111–123
120–134
5
4
132–138
135–145
142–156
5
0
104–115
113–126
122–137
5
5
134–140
137–148
144–160
5
1
106–118
115–129
125–140
5
6
136–142
139–151
146–164
5
2
108–121
118–132
128–143
5
7
138–145
142–154
149–168
5
3
111–124
121–135
131–147
5
8
140–148
145–157
152–172
5
4
114–127
124–138
134–151
5
9
142–151
148–160
155–176
5
5
117–130
127–141
137–155
5
10
144–154
151–163
158–180
5
6
120–133 130–144
140–159
5
11
146–157 154–166
161–184
5
7
123–136 133–147
143–163
6
0
149–160
157–170
164–188
5
8
126–139 136–150
146–167
6
1
152–164 160–174
168–192
5
9
129–142 139–153
149–170
6
2
155–168 164–178
172–197
5
10
132–145 142–156
152–173
6
3
158–172 167–182
176–202
5
11
135–148 145–159
155–176
6
4
162–176 171–187
181–207
6
0
138–151 148–162
158–179
—
209
—
210
— Appendixes
To Make an Approximation of Your Frame Size . . . Extend your arm and bend the forearm upward at a 90 degree angle. Keep fingers straight and turn the inside of your wrist toward your body. If you have a caliper, use it to measure the space between the two prominent bones on either side of your elbow. Without a caliper, place thumb and index finger of your other hand on these two bones. Measure the space between your fingers against a ruler or tape measure. Compare it with these tables that list elbow measurements of medium-frameed men and women. Measurements lower than those listed indicate you have a small frame. Higher measurements indicate a large frame.
Height in 1″ heels Men
Elbow Breadth
5′2″–5′3″
2½″–2⅞″
5′4″–5′7″
2⅝″–2⅞″
5′8″–5′11″
2¾″–3″
6′0″–6′3″
2¾″–3⅛″
6′4″
2⅞″–3¼″
Women 4′10″–4′11″
2¼″–2½″
5′0″–5′3″
2¼″–2½″
5′4″–5′7″
2⅜″–2⅝″
5′8″–5′11″
2⅜″–2⅝″
6′0″
2½″–2¾″
A P P E N D I X 18
Abstract from “Phenomenal and Nonphenomenal Body Image Tasks in the Treatment of Eating Disorders”
The study (PNBIT) systematically explored phenomenal and nonphenomenal body image tasks in eating disorders. Eleven prescriptive tasks including six art therapy techniques were individually administered and repeated in twenty-two sessions. Art productions were used to explore dynamics of eating disorders, especially related to body image projections. Subjects included three anorectic and three obese white women between 25 and 50 years old, not in treatment for psychological adjustment problems. The Tennessee Self Concept Scale (TSCS) was used as a verbal pre and posttest with the six research subjects and with three normal weight subjects. The PNBIT was also administered to the normal weight subjects. A nonparametric statistical analysis using the Mann-Whitney U Test for Two Independent Samples found there was a greater increase in the TSCS Total Positive Scores in the research subjects than in the normal weight subjects. Other discursive measures were self reports and an Eating Questionnaire. Seven judges evaluated thirty-six coded raw drawings for aesthetic quality and for psychological health. A nonparametric statistical analysis of the judges’ ratings using the Wilcoxin Matched-Pairs SignedRanks Test found agreement that the research subjects’ second renderings of the Body Contour Drawing task improved over the first, and was correlated chronologically both in psychological health, and in aesthetic —
211
—
212
— Appendixes
quality. Six single case studies were prepared and analyzed from verbal and nonverbal perspectives. The results indicated: (a) five of the six research subjects improved in positive self concept, (b) the PNBIT was the instrument which affected the positive change in self concept in five of the six research subjects, (c) the six research subjects demonstrated clinical gains in self management of their eating problems. Implications were drawn for the value of the aesthetic form of art therapy productions as an index to the psychological health of the individuals who produced them. Recommendations were made for the wider use of art therapy both in traditional research designs and as an integral part of a team approach to treatment of eating disorders. Thirty-eight of the subjects’ expressive art productions were reproduced.
A P P E N D I X 19
The Scope of Art Therapy
MATERIALS
MEDIA
AGE
PLACE
Paint
Painting
Children
Hospitals
Crayons
Drawing
Adolescents
Pastels
Sculpture
Adults
Day treatment rehabilitation centers
Felt tip markers
Collage
Elderly
Clay
Hospices Long-term nursing homes Prisons Normal school settings: all ages Methadone clinics Alcohol clinics Mental health centers Private practice
—
213
—
214
— Appendixes
PRACTICE
POPULATIONS
TECHNIQUES
Primary
Anorexia
Chromatic Family Line Drawing
Co-therapist
Obesity
Mandala
Consultation
Alcoholism
Lifeline
3-way treatment
Drug use disorder
Family Clay Sculpture
Diversified team
Alzheimer’s disease
Sandworlds
Schizophrenia
House/Tree/Person/Person/Animal
Depression
Body Contour Drawing
Terminally ill
Self Box
Deaf
Spontaneous drawing
Blind
Guided imagery
Stroke victim
Photography
Amputee
Printmaking
Learning impaired
Tape recording/Video taping
Sexual abuse
Mirror work
Physical abuse
Body dimension assessment
Cerebral palsy
Poetry
Suicidal
Kite making/Flying
Creative block
Working with stones/Keys/Found objects
Aphasic Cancer Relationship problems Bibliotherapy USE Diagnosis Therapeutic treatment Expressive communication Research
Dream work Mural work Journal keeping
APPENDIX 20
Relationship of Issues in Eating Disorders
ANOREXIA NERVOSA DE DE PE TO N XI DE FI N CA CY TI YO O D N -Y EN O IA L SY O F N N D EE RO DS M
E
OBESITY
FEAR OF THIN HUNGER (Fear of Deprivation) (Lack of Self Worth)
FAT
THIN
FEAR OF FAT HUNGER (Fear of Satiation) (Lack of Self Worth)
BULIMIA IMMOBILIZATION BULIMIA FEAR OF LOSS OF CONTROL—GORGING—PURGING
AN ORE XI A N ERVOSA
OBESITY N DS O EE TI N A F IC O IF L OX IA T N DE DE E M CY N O E R D D N N PE SY DE
YO
-Y
OUT OF CONTROL—EMOTIONS AND WORLD
OUT OF CONTROL—EMOTIONS AND WORLD
BULIMIA
O
—
215
—
A P P E N D I X 21
Figure Selection II
INSTRUCTIONS: Circle the drawing which best represents your figure at this time.
Name ___________________ Date ____________________
—
216
—
APPENDIX 22
Color Chart
COLOR CHART NAME __________ DATE _______ RED
ORANGE
YELLOW
GREEN
BLUE
VIOLET
BLACK WHITE
—
217
—
APPENDIX 23
Tissue Box Estimate
Name _________________________________
Date ____________________
INSTRUCTIONS: Estimate height, width and depth of the tissue box in inches:
Depth
Height
Width
—
218
—
REFERENCES
Alexander, F. 1950. Psychosomatic Medicine: Its Principles and Applications. New York: Norton. Anderson, A. 1990. Males with Eating Disorders. New York: Brunner/Mazel. American Psychiatric Association. 1980. Diagnostic and Statistical Manual of Mental Disorders 3d ed. Washington, D.C.: American Psychiatric Association. Arieti, S. 1976. Creativity, the Magic Synthesis. New York: Basic. Baumeister, A. A. 1967. Problems of comparative studies of mental retardates and normals. American Journal of Mental Deficiency, 71:869–875. Becker, E. 1973. The Denial of Death. New York: Free. Bell, C. 1958 [1913]. Art. New York: Capricorn. Bell, R. 1986. Holy Anorexia. Chicago: University of Chicago Press. Berlyne, D. E. 1974. Studies in the New Experimental Aesthetics: Steps Toward an Objective Psychology of Aesthetic Appreciation. Washington, D.C.: Hemisphere. Bilich, M. 1983. Weight Loss from the Inside Out. New York: Seabury. Brecher, E. and Editors of Consumer Reports. 1972. Licit and Illicit Drugs. Boston: Little, Brown. Brody, J. E. 1985. Panel finds obesity a major U.S. killer in need of attention. New York Times, February 14. ——— 1986, January 23. Fat or fit? Study may confirm suspicions it is the genes. New York Times, A24. Bruch, H. 1973. Eating Disorders: Obesity, Anorexia Nervosa, and the Person Within. New York: Basic Books. ——— 1978. The Golden Cage. Cambridge: Harvard University Press. ——— 1982. Anorexia nervosa: Therapy and theory. American Journal of Psychiatry 139(12): 1531–1538. Bruscia, K. E. 1979. Auditory short-term memory and selective attention among the mentally retarded. Ph.D. diss., New York University. Buck, J. N. and E. Hammer. 1969. Advances in the House-Tree-Person Technique: Variations and Applications. Los Angeles: Western Psychological Services. Burns, R. C. and S. Kaufman. 1972. Actions, Styles, and Symbols in Kinetic Family Drawings (K-F-D). New York: Brunner/Mazel. Cane, F. 1951. The Artist in Each of Us. New York: Pantheon. Cannman, W. J. N.d. The stigma of overweight: Six autobiographies. Unpublished manuscript.
—
219
—
220
— References
Casper, R. C., D. Offer, and E. Ostrov. 1981. The self image of adolescents with acute anorexia nervosa. Journal of Pediatrics 98(4): 656–661. Chesler, P. 2001. Woman’s Inhumanity to Woman. New York: Thunder’s Mouth. Chodil, J. J. 1978. An Investigation of the Relation Between Perceived Body Space, Actual Body Space, Body Image Boundary, and Self-Esteem. New York: New York University. Cirlot, J. E. 1971. A Dictionary of Symbols. 2d ed. Trans. J. Sage. New York: Philosophical Library. Crisp, A. H. 1980. Anorexia Nervosa: Let Me Be. London: Academic. Crisp, A. H., J. H. Kalucy, and B. Harding. 1977. The long-term prognosis in anorexia nervosa: Some factors predictive of outcome. In R. A. Vigersky, ed., Anorexia Nervosa, pp. 55–65. New York: Raven. Crowl, M. 1980. Art therapy with patients suffering from anorexia nervosa. Arts in Psychotherapy 7(2): 141–151. Elin, N. and A. O. Nucho. 1979. The use of kinetic family drawings as a diagnostic tool in assessing the child’s self-concept. Art Psychotherapy 6:241–247. Estrich, S. 2001. Sex and Power. New York: Riverhead. Fairweather, P. D. with D. Johnson. 1981. Symbolic Regression Psychology. New York: Irvington. Fisher, S. and S. Cleveland. 1968. Body Image and Personality. New York: Dover. Fitts, W. H. 1965. Tennessee Self Concept Scale. Nashville: Counselor Recordings and Tests. ——— 1972. The Self Concept and Psychopathology. Monograph 4. Nashville: Dede Wallace Center. Fitts, W. H., Adams, J. L., Radford, G., Richard, W. C., Thomas, B. K., Thomas, M. M., and Thompson, W. 1971. The Self Concept and Self-Actualization. Monograph 3. Nashville: Dede Wallace Center. Frank, L. K. 1959. Projective methods for the study of personality. Journal of Psychology 8(409): 389–409. Freud, S. 1927. The Ego and the Id. London: Hogarth. Friedan, B. 2001. The Feminine Mystique. New York: Norton. Gantt, L. 1979. The other side of art therapy. American Journal of Art Therapy 19(1): 11–18. Garfinkel, P. E., and D. M. Garner. 1982. Anorexia Nervosa: A Multidimensional Perspective. New York: Brunner/Mazel. Gellert, E. N.d. Bibliography of the literature on body image. Unpublished manuscript. ——— 1967. Supplement to the bibliography of the literature on body image. Unpublished manuscript. ——— N.d. Supplement 2 to the bibliography of the literature on body image. Unpublished manuscript. Glucksman, M. L., J. Hirsch, R. S. McCully, B. A. Barron, and J. L. Knittle. 1968. The response of obese patients to weight reduction 11. A quantitative evaluation of behavior. Psychosomatic Medicine 30(4): 359–373. Goldfarb, W. 1964. Childhood Schizophrenia: International Psychiatry Clinics 1:821–845.
References — 221 Gombrich, E. H. 1960. Art and Illusion. Princeton: Princeton University Press. Goodman, M., and B. Kotkov. 1953. Prediction of trait ranks from draw-a-person measurements of obese and non-obese women. Journal of Clinical Psychology 9:365–367. Halmi, K. A., S. C. Goldberg, E. Eckert, R. Casper, and J. M. Davis. 1977. Pretreatment evaluation in anorexia nervosa. In R. A. Vigersky, ed., Anorexia nervosa, pp. 43–54. New York: Raven. Hammer, E. 1958. The Clinical Application of Projective Drawings. Springfield, Ill.: Thomas. Hatterer, L. J. 1980. The Pleasure Addicts: The Addictive Process—Food, Sex, Drugs, Alcohol, Work, and More. Cranbury, N.J.: Barnes. Hinsie, L. E., and R. J. Campbell. 1970. Psychiatric Dictionary. New York: Oxford University Press. Hirschhorn, K. 1982. Letter to Robert J. Haggerty, William T. Grant Foundation, New York, February. Hoff Sommers, C. 1995. Who Stole Feminism? New York: Simon and Schuster. Huebner, H. 1985. Anorexia and bulimia: An addiction to the body’s natural painkiller [Summary]. Proceedings of Conference on Anorexia and Bulimia: New Directions in Education, Diagnosis and Treatment 8(3): 7. Jeffrey, R. W., Wing, R. R., and Stunkard, A. 1978. Behavioral treatment of obesity: The state of the art 1976. Behavior Therapy 9(2): 189–199. Jung, C. G. 1931. Psychology of the Unconscious. New York: Dodd/Mead. ——— 1959. Mandala Symbolism. Trans. R. F. C. Hull. Princeton: Princeton University Press. Kalff, D. 1980. Sandplay. Santa Monica: Sigo. Kaplan, L. J. 1978. Oneness and Separateness: From Infant to Individual. New York: Touchstone. Kellogg, J. 1981. Mandala, Path of Beauty. Towson, Md.: Mandala Assessment and Research Center. Kestenberg, J. S. 1967. The role of movement patterns in development. Part 3: The control of shape. Psychoanalytic Quarterly 36(3): 356–409. Kleges, R. C. 1983. An analysis of body image distortions in a nonpatient population. International Journal of Eating Disorders, 2(2): 35–41. Klingman, M. 1981. The Secret Lives of Fat People. Boston: Houghton Mifflin. Knittle, J. L. 1972. Obesity in childhood: A problem in adipose tissue cellular development. Journal of Pediatrics 81(6): 1048–1059. Knittle, J. L., ed. 1986. Nutrition Syllabus. New York: Mt. Sinai School of Medicine, City University of New York. Knittle, J. L., K. I. Timmers, and D. Katz. 1982. Adolescent obesity. In Myron Winick, ed., Adolescent Nutrition, pp. 151–165. New York: Wiley. Koppitz, E. M. 1968. Psychological Evaluation of Children’s Human Figure Drawings. New York: Grune and Stratton. Kramer, E. 1971. Art as Therapy with Children. New York: Schocken.
222
— References
Kwiatkowska, H. 1978. Family Therapy and Evaluation Through Art. Springfield, Ill.: Thomas. Langer, Suzanne K. 1942. Philosophy in a New Key: A Study in the Symbolism of Reason, Rite, and Art. Cambridge: Harvard University Press. ——— 1957. Problems of Art. New York: Scribner’s. Lettieri, R. J. 1983. Consciousness, self-deception, and psychotherapy: An analogue study. Imagination, Cognition, and Personality 3(2): 83–97. Levenkron, S. 1982. Treating and Overcoming Anorexia Nervosa. New York: Scribner’s. Machover, K. 1949. Personality Projection. Springfield, Ill.: Thomas. Mahler, M., F. Pine, and A. Berman. 1967. On Human Symbiosis and the Vicissitudes of Individuation. Vol. 1: The Psychological Birth of the Human Infant. New York: Basic. Marasciulo, L. A. and M. McSweeney. 1977. Nonparametric and Distribution-Free Methods for the Social Sciences. Monterey: Brooks/Cole. Marrazzi, M. A. and E. D. Luby. 1986, February. An auto-addiction opioid model of chronic anorexia nervosa. International Journal of Eating Disorders 5(2): 191–208. Maslow, A. 1968. Toward a Psychology of Being. 2d ed. New York: Van Nostrand. May, R. 1975. The Courage to Create. New York: Norton. Menaker, E. 1985, Summer. The concept of will in the thinking of Otto Rank and its consequences for clinical practice. Psychoanalytic Review 72(3): 255–264. Millman, M. 1980. Such a Pretty Face. New York: Norton. Mitchell, D. 1980. Anorexia nervosa. Arts in Psychotherapy 7(1): 53–60. Mrosovsky, N., and Sherry, D. F. 1980. Animal anorexias. Science 207:837–841. National Clearinghouse for Mental Health Information, Division of Scientific and Public Information, and R. W. Moore. 1981. Art Therapy in Mental Health. Rockville, Md.: U.S. Dept. of Health and Human Services. Naumburg, M. 1973. An Introduction to Art Therapy: Studies of “Free Art Expression of Behavior Problem Children and Adolescents as a Means of Diagnosis and Therapy. New York: Teachers College Press. ——— 1987 [1966]. Dynamically Oriented Art Therapy: Its Principles and Practice. Chicago: Magnolia Street Naumburg, M. and J. Caldwell. 1957. The use of spontaneous art in analytically oriented group therapy of obese women. Acta Psychotherapy 7(Supplement): 254– 287. Neuman, P., and P. A. Halvorson. 1983. Anorexia Nervosa and Bulimia: A Handbook for Counselors and Therapists. New York: Van Nostrand Reinhold. Norris, D. L. 1984. The effects of mirror confrontation on self-estimation of body dimensions in anorexia nervosa, bulimia and two control groups. Psychological Medicine 14: 835–842. Orbach, S. 1978. Fat Is a Feminist Issue. New York: Berkley. Pope, G., K. Phillips, and R. Olivardia. 2000. The Adonis Complex: The Secret Crisis of Male Body Obsession. New York: Free. Powers, S., and J. Langworthy. 1978. Art work: Another dimension in the treatment of psychiatric patients. Art Psychotherapy 5(2): 71–79.
References — 223
Rabin, M. 1977. The yo-yo in art therapy: The use of art therapy in eating disorders. Master’s thesis, College of New Rochelle, New York. ——— 1987. Phenomenal and nonphenomenal body image tasks in the treatment of eating disorders. Ann Arbor: University Microfilms International. ——— 1993. Full circle. Art Therapy: Journal of the American Art Therapy Association 10(3): 171–172. Rank, O. 1929. The Trauma of Birth. New York: Harcourt, Brace. Reed, P., W. H. Fitts, and L. Boehm. 1981. Tennessee self concept scale bibliography of research studies. Rev. ed. Los Angeles: Western Psychological Services. Reich, W. 1949. Character Analysis. New York: Orgone Institute Press. Robbins, A. and L. Sibley. 1976. Creative Art Therapy. New York: Brunner/Mazel. Rogers, C. 1959. Theory of therapy, personality, and interpersonal relationships as developed in the client-centered framework. In S. Koch, ed., Psychology: A Study of a Science. Vol. 3: Formulation of the Person and the Social Conflict, pp. 184–256. New York: McGraw-Hill. ——— 1961. On Becoming a Person. Boston: Houghton Mifflin. Rose, G. 1981. The Power of Form: A Psychological Approach to Aesthetic Form. New York: International Universities Press. Schilder, P. 1953. The Image and Appearance of the Human Body. London: Paul Kegan, Trench, Trubner. Siegel, S. 1956. Nonparametric Statistics for the Behavioral Sciences. New York: McGrawHill. Sorensen, T. I. A., A. J. Stunkard, W. Teasdale, and M. W. Higgins. 1983. The accuracy of weight: children’s recall of their parents weights fifteen years earlier. International Journal of Obesity 7: 115–122. Steinem, Gloria. 1995. Outrageous Acts and Everyday Rebellions. 2d ed. New York: Holt. Stevens, A. 1983. Archetypes: A Natural History of the Self. New York: Quill. ——— 1994. Jung. 2d ed. New York: Barnes and Noble. Storr, A. 1989. Freud. New York: Barnes and Noble. Thompson, W. 1972. Correlates of the self concept. Studies on the self concept. Monograph 6. Nashville: Counselor Recordings and Tests. Tolor, A. and P. V. Digrazia. 1977. The body image of pregnant women as reflected in their human figure drawings. Journal of Clinical Psychology 33(2): 566–571. Touyz, W., P. J. V. Beamont, J. K. Collins, and I. Cowie. 1985, August. Body shape perception in bulimia and anorexia nervosa. International Journal of Eating Disorders 4(3): 259–265. Wadeson, H. 1980. Art Psychotherapy. New York: John Wiley. Wadeson, H., ed. 1986. Art therapy expert witness. American Art Therapy Association Newsletter 6(2): 5–6. Weller, I., T. Arad, and R. Levit. 1977. Self concept, delayed gratification, and field dependence of successful and unsuccessful dieters. Israel Annals of Psychiatry and Related Disciplines 15(1): 41–46. Weiner, H. 1985, November. The physiology of eating disorders. International Journal of Eating Disorders 4(4): 347–388.
224
— References
Wolf, J. M., M. E. Wilmuth, T. Gazda, and A. Watkins. 1985, May. The role of art in the therapy of anorexia nervosa. International Journal of Eating Disorders 4(2): 185–200. Woodman, M. 1980. The Owl Was a Baker’s Daughter, Anorexia Nervosa, and the Repressed Feminine. Toronto: Inner City. Woods, W. P., and D. M. L. Heretick. 1983–1984. Self-schemata in anorexia and obesity. Imagination, Cognition, and Personality 3(1): 31–48. Wylie, R. C. 1961. The Self Concept. Lincoln: University of Nebraska Press.
INDEX
abortion, 16–17 addiction: dual nature of, 27; in eating disorders, 1–2, 11, 153; fluid nature of, 151; self-concept and body image in, 153 adolescence, 153 Adonis complex, 14 The Adonis Complex (Pope, Phillips, and Olivardi), 14, 20 age, Claudia Bernard lies about, 88, 93 Alexander, Jane, 161 Allen (Heather) case study, see Heather Allen case study anger, of Linda Miller, 146–47 animal drawings, see House/Tree/ Person/Person (Opposite Sex)/ Animal (HTPPA) drawings anorexia nervosa: addiction in, 2, 147, 153; among college students, 8; among nuns, 7–8; body image in, 1, 12–13; definition of, 7; diagnostic classification of, 7; diet effectiveness in, 9–10; Heather Allen case study, 106–26; history of, 7–8; Linda Miller case study, 126–49; self-nurturing ability in, 11; treatment of, 8 appetite, 2 archetypes, 19–20 art: ethical society and, 161–63; as index to psychological health, 4–5; search for form in, 4–5; social function of, 160–61 art therapy: acceptance as legitimate discipline, xiii, 23, 160–61; art of, 163; basis for, 22–23; dream work in, 24–25; dynamics of, 6; establishing freedom in, 28; gender bias in, 151– 52; interpretation in, 25; multidimensional nature of, xiii; progress prediction in, 26; as scientific evidence, 149; scope of, 213–14;
socialization and, xii; suicidal images in, 207–8; therapeutic effectiveness of, 26, 156, 158–59; therapy of, 22–26; unconscious and, 6, 24–26; verbalization in, xi–xiii, 23–24 BCD, see body contour drawings (BCD) BDEM, see body dimension estimate and measurements (BDEM) beauty, 6–7 Bell, C., 4–5 Bell, R., 7 Bellafonte, Ginia, 15 Bernard (Claudia) case study, see Claudia Bernard case study biological clock: Claudia Bernard and, 93, 96; Linda Miller and, 141 body contour drawings (BCD), 40–42; Claudia Bernard case study, 101, 102f; Heather Allen case study, 121–22, 122f; Jessica Mason case study, 83–84, 84f; Linda Miller case study, 141–45, 142f; Megan Brown case study, 61–64, 62f; questionnaire, 41, 200–1; subjects’ reaction to, 143–44; therapeutic use of, 158 body dimension estimate and measurements (BDEM), 30–31; circumference, female, 193–94; circumference, male, 189–90; Claudia Bernard case study, 93; figure selection chart, 216; frame size estimate chart, 210; Heather Allen case study, 112; inaccurate perception of, 144; Jessica Mason case study, 74–75; Linda Miller case study, 133; linear, female, 191–92; linear, male, 187–88; Megan Brown case study, 51; Metropolitan Life Insurance height and weight tables, 209 body dysmorphic disorder, 14
—
225
—
226
— Index
body image: American ideal of, 6–10; body dimension estimates vs. actual measurements, 30–31; definition of, 2; distortion of, 12–14, 152; genetic templates and, 6; in males, 14–15; nonphenomenal, defined, 3; PNBIT in development of, 156, 158; self and, 11–21; self-concept and, 13–14, 153; significance of, 1–10; thinness as ideal, 6–7; yo-yo syndrome in, 17 brain function, 22 Brown (Megan) case study, see Megan Brown case study Bruch, H., 9 bulimia, 154 caloric restriction, 11 Campbell, R. J., 129, 139 Carpenter, Karen, 7 case studies, see clinical applications Catherine de Siena (saint), 8 Chesler, P., 17 Chromatic Family Line Drawing (CFLD), 32–33; Claudia Bernard case study, 94; Heather Allen case study, 112–14, 113f; Jessica Mason case study, 75, 76f; Linda Miller case study, 133; Megan Brown case study, 52 Cirlot, J. E., 78, 140 Claudia Bernard case study, 44–67; biological clock in, 93, 96; body contour drawings, 101, 102f; body dimension estimates and measurements, 93; chromatic family line drawings, 94; discussion of, 103, 105; eating questionnaire, 104; exit tape recording extract, 168–69; family history, 91; HTPPA drawings, 94–96; kinetic family clay sculpture, 100–1; lies about age, 88, 93; mandalas, 96–99, 97f, 98f, 99f; medical history, 90–91; mirror viewing, face, 92; mirror viewing, full-length, 92–93; nonphenomenal tasks, 94–101; personal history, 90; phenomenal tasks, 92–93; project compliance, 91–92; Sandworlds, 100; Self Box, 99–100; self report, 102–3; summary, 105–6; Tennessee Self Concept Scale data analysis, 87–88, 89f, 90; weight history, 90; weight recording, 92
clinical applications, 43–150; Claudia Bernard case study, 44–67; Heather Allen case study, 106–26; Jessica Mason case study, 68–87; Linda Miller case study, 126–49; Megan Brown case study, 44–67 clothing industry: acknowledgment of large-sized customers, 10; September 11 disaster impact on, 14–15; thinness ideal and, 7 colleges, eating disorder prevention in, 155–56 college students, eating disorders in, 154 color chart form, 31, 217 combined phenomenal and nonphenomenal task: body contour drawing, 3, 40–42; Claudia Bernard case study, 101, 102f; Heather Allen case study, 121–22, 122f; Jessica Mason case study, 83–84, 84f; Linda Miller case study, 141–43, 142f; Megan Brown case study, 61–64, 62f corpus callosum, 22 creativity, brain function in, 22 cultural elitism, 161 Diagnostic and Statistical Manual of Mental Disorders (DSM-III), 7 Doolittle, John T., 161 drawing techniques, projective, 37 dreams, 24–25 Dynamically Oriented Art Therapy: Its Principles and Practice (Naumburg), xii eating disorders: addiction in, 1–2; body image in, 12–14; caloric restriction in, 11; in college students, 154; female bias in research on, 151–52; in males, 14, 20; relationship of issues in, 215; school prevention programs, 155–56; yo-yo syndrome in, 9 eating questionnaire, 196–200; Claudia Bernard case study, 104; Heather Allen case study, 124t; Jessica Mason case study, 85, 85t; Linda Miller case study, 146t; Megan Brown case study, 65t–66t elitism, cultural, 161
Index — 227
endogenous opioids, in appetite regulation, 2 estimates, see body dimension estimate and measurements Estrich, S., 17 ethical society, art and, 161–63 exercise, 14 family role, in eating disorders, 152, 153–54 fashion industry, see clothing industry fat advocacy groups, 10 feeding of infants, 11 females: circumference, body dimension estimate and measurements, 193–94; gender bias in eating disorder research, 151–52; linear, body dimension estimate and measurements, 191–92; outline drawings, figure selection, 186; weight ranges in, 18f feminazi, 17 The Feminine Mystique (Friedan), 15, 17 feminism: backlash against, 16–17; gender relations in, 16; growth of, 15–17 food: addiction to, 2; as reward, 129 form: concept of, 4–5; meaningful, as psychotherapeutic goal, 4 frame size estimate chart, 210 Freud, Sigmund, 19, 24 Friedan, Betty, 15–16, 17–19, 20 Gantt, L., 26 gender roles: female bias in eating disorder research, 151–52; feminism and, 16, 18–19, 20 Goldfarb, W., 13 Gombrich, E. H., 13, 143 Hackney, Sheldon, 161 Hammer, E., 34 Hatterer, L. J., 1–2, 12 health, definition of, 4 Heather Allen case study, 106–26; body contour drawings, 121–22, 122f; body dimension estimates and measurements, 112; chromatic family line drawing, 112–14, 113f; discussion of, 123, 125; eating questionnaire, 124t; exit tape recording extract, 168–72; family history, 110; HTPPA drawings, 114–17, 116f; kinetic family clay sculp-
ture, 120; mandalas, 117–18, 119f; medical history, 110; mirror viewing, face, 112; mirror viewing, full-length, 112; nonphenomenal tasks, 112–20; personal history, 108; phenomenal tasks, 111–12; project compliance, 110–11; Sandworlds, 120; Self Box, 118, 120; self report, 122–23; summary, 125–26; Tennessee Self Concept Scale data analysis, 106, 107f, 108; weight history, 108–9; weight recording, 111–12 height and weight tables, 209 heroes, of September 11 disaster, 15 Hinsie, L. E., 129, 139 Holy Anorexia (Bell), 7 House/Tree/Person/Person (Opposite Sex)/Animal (HTPPA) drawings, 33–37; Claudia Bernard case study, 94–96; Heather Allen case study, 114–17, 116f; Jessica Mason case study, 72, 73f, 75, 77–79, 77f, 80f; Linda Miller case study, 133–35; Megan Brown case study, 52–53, 54f, 55–56, 55f illusion, mirror image as, 143–44 infant feeding and nurture, 11 Jenny Craig weight loss program, 8 Jessica Mason case study, 68–87; body contour drawings, 83–84, 84f; body dimension estimates and measurements, 74–75; chromatic family line drawing, 75, 76f; discussion of, 85– 86; eating questionnaire, 85, 85t; exit tape recording extract, 165–68; family history, 70–71; HTPPA drawings, 72, 73f, 75, 77–79, 77f, 80f; kinetic family clay sculpture, 81–83; mandalas, 79; medical history, 70; mirror viewing, face, 72–73; mirror viewing, fulllength, 73–74; nonphenomenal tasks, 75–83; personal history, 70; phenomenal tasks, 71–75; project compliance, 71; Sandworlds, 81; Self Box, 81, 82f; self report, 84–85; strabismus in, 72; summary, 86–87; Tennessee Self Concept Scale data analysis, 68, 69, 69f; weight history, 70; weight recording, 71–72 Jung, C. G., 19–20, 163
228
— Index
Kalff, D., 39 Kaplan, L. J., 85, 86 kinetic family clay sculpture (KFCS), 40; Claudia Bernard case study, 100–1; Heather Allen case study, 120; Jessica Mason case study, 81–83; Linda Miller case study, 141; Megan Brown case study, 60–61, 61f Knittle, J. L., 9 Kramer, E., 161 Langer, Suzanne K., 5, 144, 158 Linda Miller case study, 126–49; anger in, 146–47; body contour drawings, 141–45, 142f; body dimension estimates and measurements, 133; chromatic family line drawing, 133; discussion of, 145–48; eating questionnaire, 146t; exit tape recording extract, 172–78; family history, 130–31; HTPPA drawings, 133–35; kinetic family clay sculpture, 141; mandalas, 135–36, 137f, 138; medical history, 130; mirror viewing, face, 132; mirror viewing, full-length, 132; nonphenomenal tasks, 133–45; personal history, 129; phenomenal tasks, 132–33; project compliance, 131–32; relationship with father, 130–31; Sandworlds, 139–41; Self Box, 138–39; self report, 145; summary, 148–49; Tennessee Self Concept Scale data analysis, 126–27, 128f, 129; weight history, 129–30; weight recording, 132 Luby, E. D., 2, 147 Machover, K., 37 males: body image distortion in, 14–15; circumference, body dimension estimate and measurements, 189–90; eating disorders in, 14, 20, 151–52; fashion industry and September 11 disaster, 15; linear, body dimension estimate and measurements, 187–88; outline drawings, figure selection, 185; weight ranges in, 19f Males with Eating Disorders (Anderson), 20 mandalas, 37–38; Claudia Bernard case study, 96–99, 97f, 98f, 99f; Heather Allen case study, 117–18, 119f; Jessica
Mason case study, 79; Linda Miller case study, 135–36, 137f, 138; Megan Brown case study, 56–59 manifest dream, 24, 35 Marrazzi, M. A., 2, 147 Maslow, A., 163 Mason (Jessica) case study, see Jessica Mason case study May, R., 4 medical questionnaire, 204 medical release form, 203 Megan Brown case study, 44–67; body contour drawings, 61–64, 62f; body dimension estimate and measurement, 51; changed appearance of, 50–51; chromatic family line drawing, 52; discussion of, 64, 66–67; eating questionnaire, 65t–66t; exit tape recording extract, 63–64; family history, 48; growing independence in, 50; HTPPA drawings, 52–53, 54f, 55–56, 55f; kinetic family clay sculpture, 60–61, 61f; mirror viewing, face, 50–51; mirror viewing, full-length, 51; nonphenomenal tasks, 52–61; personal history, 45, 46, 47–48; phenomenal tasks, 50–51; physical description, 45; project compliance, 48–49; Sandworlds, 59–60, 60f; Self Box, 58–59; self report, 63–64; summary, 67; Tennessee Self Concept Scale data analysis, 44–45, 46f; weight history, 47; weight recording, 50 Metropolitan Life Insurance height and weight tables, 209 Miller (Linda) case study, see Linda Miller case study mirror image, 13, 143–44 mirror viewing, face, 30; Claudia Bernard case study, 92; Heather Allen case study, 112; Jessica Mason case study, 72–73; Linda Miller case study, 132; Megan Brown case study, 50–51 mirror viewing, full-length, 30; Claudia Bernard case study, 92–93; Heather Allen case study, 112; Jessica Mason case study, 73–74; Linda Miller case study, 132; Megan Brown case study, 51 My Fair Lady (Lerner and Lowe), 21
Index — 229
National Endowment for the Arts, 161 National Endowment for the Humanities, 161 Naumburg, Margaret, xii, 25, 26 night-eating syndrome, 129 nonphenomenal body image, 3 nonphenomenal tasks: Claudia Bernard case study, 94–101; definition of, 3; Heather Allen case study, 112–20; house/tree/person/person (opposite sex)/animal drawings, 33–37; Jessica Mason case study, 75–83; Kinetic Family Clay Sculpture, 40; Linda Miller case study, 133–45; mandalas, 37–38; Megan Brown case study, 52–61; Sandworlds, 39; self box, 38–39; self concept development through, 157t; see also specific tasks normal weight, defined, 3 Norris, D. L., 143, 144 Nutrisystem, 8 obesity: body image distortion in, 9, 12–13; body image tasks in, 1; Claudia Bernard case study, 87–106; complications of, 8; diet effectiveness in, 9–10; as epidemic, 8; fat advocacy groups and, 10; food addiction in, 2, 153; Jessica Mason case study, 68–87; Megan Brown case study, 44–67; prevalence of, 8; self-nurturing ability in, 11 Olivardi, R., 14 opioids, endogenous, 2 opposite sex person drawings, see House/Tree/Person/Person (Opposite Sex)/Animal (HTPPA) drawings Optifast diet, 8 outline drawings: in body dimension estimates, 30; figure selection, female, 186; figure selection, male, 185 Overeaters Anonymous, 8 parents, as role models, 154 person drawings, see House/Tree/ Person/Person (Opposite Sex)/Animal (HTPPA) drawings Phenomenal and Nonphenomenal Body Image Tasks (PNBIT): abstract
of study, 211–12; art therapy session, 27–28; case studies, 43–150; Claudia Bernard case study, 87–106; clinical effectiveness of, 42; combined phenomenal and nonphenomenal task, 40–42; definition of, 3; Heather Allen case study, 106–26; Jessica Mason case study, 68–87; Linda Miller case study, 126–48; materials and equipment, 29; Megan Brown case study, 44–67; methodology of, 27–42; nonphenomenal tasks, 32–40; parts of, 28; phenomenal tasks, 29–31; self-concept and, 152; similarities in case studies, 149; therapeutic effectiveness of, 156, 158; uses for, 2, 150 phenomenal body image, 3 phenomenal tasks: body dimension estimates and measurements, 30–31; Claudia Bernard case study, 92–93; definition of, 3; Heather Allen case study, 111–12; Jessica Mason case study, 71–75; Linda Miller case study, 132–33; Megan Brown case study, 50–51; mirror viewing, face, 30; mirror viewing, full-length, 30; self concept development through, 157t; weight recording, 29–30; see also specific tasks Phillips, K., 14 Playboy bunnies, 16, 17 PNBIT, see Phenomenal and Nonphenomenal Body Image Tasks (PNBIT) Pope, G., 14 postdrawing interrogation, 34–36 Prince Charming, as rescuer, 93, 96 printmaking, 163 projective drawing techniques, 37 psychotherapy, meaningful form in, 4 Pygmalion (Shaw), 21 questionnaires: body contour drawing, 41, 200–1; medical, 204; self box, 201–2 Quindlen, Anna, 17 Rabin, M., 161–62 relief print, 163 Robbins, A., 39 Rogers, C., 4, 145
230
— Index
safe haven, 28 Sandworlds, 39; Claudia Bernard case study, 100; grid, 195; Heather Allen case study, 120; Jessica Mason case study, 81; Linda Miller case study, 139–41; Megan Brown case study, 59–60, 60f Satcher, Richard, 8 scarecrow, 140, 145 schizophrenia, body image in, 13 schools, and eating disorder prevention, 155–56 self: body image and, 11–21; definition of, 3 Self Box, 38–39; Claudia Bernard case study, 99–100; Heather Allen case study, 118, 120; Jessica Mason case study, 81, 82f; Linda Miller case study, 138–39; Megan Brown case study, 58–59; questionnaires, 201–2 self-concept: body image and, 13–14; definition of, 3; development of, 153, 157t; need to acknowledge, xi; PNBIT and, 152; weight changes and, 6 self-esteem, xi, 3 self-management, in weight loss, 12 self-nurture, 11 self report: Claudia Bernard case study, 102–3; form for, 28, 179–80; Heather Allen case study, 122–23; Jessica Mason case study, 84–85; Linda Miller case study, 145; Megan Brown case study, 63–64 September 11, 2001 disaster, 14–15 Sequence and Time Chart, 28, 29, 183–84 Shaw, George Bernard, 21 Sibley, L., 39 Silver Cord Syndrome, 139 smoking, weight gain and, 12 solar dreams, 6, 24–26 Somers, Hoff, 17 spiral, symbolism of, 207 Steinem, Gloria, 16–17 stereotypes, feminist impact on, 16, 18–19, 20 steroid abuse, 14 Stevens, A., 19–20, 44 Stillman Diet, 70 strabismus, 72
suicide, art therapy images and, 207–8 support groups, failure of, 153 symbolic transformation, 144 tape recording extracts: Claudia Bernard case study, 168–69; Heather Allen case study, 169–72; Jessica Mason case study, 165–68; Linda Miller case study, 172–78; Megan Brown case study, 63–64 Tennessee Self Concept Scale (TSCS): Claudia Bernard data analysis, 87–88, 89f, 90; definition of, 3; Heather Allen data analysis, 106, 107f, 108; Jessica Mason data analysis, 68, 69, 69f; Linda Miller data analysis, 126–27, 128f, 129; Megan Brown data analysis, 44–45, 46f; use in PNBIT protocol, 126 therapeutic community: attitude toward art therapy, xiii, 23, 160–61 Therapist Report, 29, 181–82 thinness, 6–7, 10 tissue box estimate, 218 transformation, symbolic, 144 tree drawings, see House/Tree/Person/ Person (Opposite Sex)/Animal (HTPPA) drawings trust, of art therapist, 27 TSCS, see Tennessee Self Concept Scale (TSCS) Twiggy, 7 unconscious, in art therapy, 6, 24–26 verbalization: in art therapy, xi–xiii, 23–24; covering up denial with, 23 violence, by students, 154–55 Wadeson, H., 207 weight: female range of, 18f; male range of, 19f; normal, defined, 3 weightlifting, 14 weight loss programs, 8–9, 11–12 weight recording, 29–30; Claudia Bernard case study, 92; Heather Allen case study, 111–12; Jessica Mason case study, 71–72; Linda Miller case study, 132; Megan Brown case study, 50
Index — 231
Weight Watchers, 8; Claudia Bernard participation in, 90; Jessica Mason participation in, 70; Megan Brown participation in, 47 Weiner, H., 1 women, see females women’s movement, 15–17 woodblock, 163 World Trade Center terrorist attack, 14–15
The Yo-Yo in Art Therapy: the Use of Art Therapy in Eating Disorders (Rabin), 205–6 yo-yo syndrome: abstract from Rabin thesis, 205–6; addiction in, 11; body image and, 17; definition of, 4; in eating disorders, 9; physiologic response to, 11 Zone (diet meal service), 9